
Prim Care Companion CNS Disord 2022;24(1):21cr03132
To cite: Spiegel DR, Ali A, Dao C, et al. Psychosis after SARS-CoV-2 in a patient with stable schizophrenia and allograft kidney transplant. Prim Care Companion CNS Disord. 2022;24(1):21cr03132.
To share: https://doi.org/10.4088/PCC.21cr03132
© Copyright 2022 Physicians Postgraduate Press, Inc.
aDepartment of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
*Corresponding author: David R. Spiegel, MD, Eastern Virginia Medical School, Department of Psychiatry and Behavioral Sciences, 825 Fairfax Ave, Norfolk, VA 23507 ([email protected]).
The coronavirus disease 2019 (COVID-19) pandemic has uprooted the lives of many individuals in its wake. Two reported groups of patients with increased vulnerability to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection are those with schizophrenia1 and solid organ transplant (SOT).2 We present the case of a patient with stabilized schizophrenia who was status post–renal transplant who subsequently acquired COVID-19. We highlight how all the conditions interacted on the course of each other.
Case Report
Ms A was a 64-year-old black woman who presented to the emergency department (ED) stating multiple paranoid delusions. Notably, she had a history of schizophrenia, insulin-dependent diabetes mellitus, and chronic kidney disease with deceased donor kidney transplant 4 years prior to presentation. By history, Ms A was fastidiously adherent to her home medication regimen, including haloperidol, mycophenolate, tacrolimus, prednisone, and insulin. She had no reported relapse of psychotic symptoms for the past 10 years, which covered pre- and post-SOT and SOT rejection. Laboratory evaluation in the ED included unremarkable complete blood count and metabolic profile except for blood urea nitrogen/creatinine = 53/3.6 mg/dL, hemoglobin A1C = 8.2%, and undetectable mycophenolic acid and tacrolimus levels. Both blood alcohol level and urine drug screen were negative.
Upon admission to the general medical floor, Ms A refused all medications except for insulin. After 2 weeks, court-committed medication treatment, including antipsychotics, was granted. At this time, the psychiatric consultation service was contacted.
Figure 13–9 details Ms A’s hospital course and posited pathophysiology of her psychosis. Notably, 9 months prior to this incident hospitalization, she developed delusions following acute COVID-19 pneumonia. The latter, which was treated on the general medical floor, required oxygen supplementation and intravenous antibiotics but no admission to the intensive care unit or mechanical ventilation. Subsequently, she became nonadherent to transplant pharmacotherapy and antipsychotics, resulting in recurrent hospitalizations for renal transplant rejection.
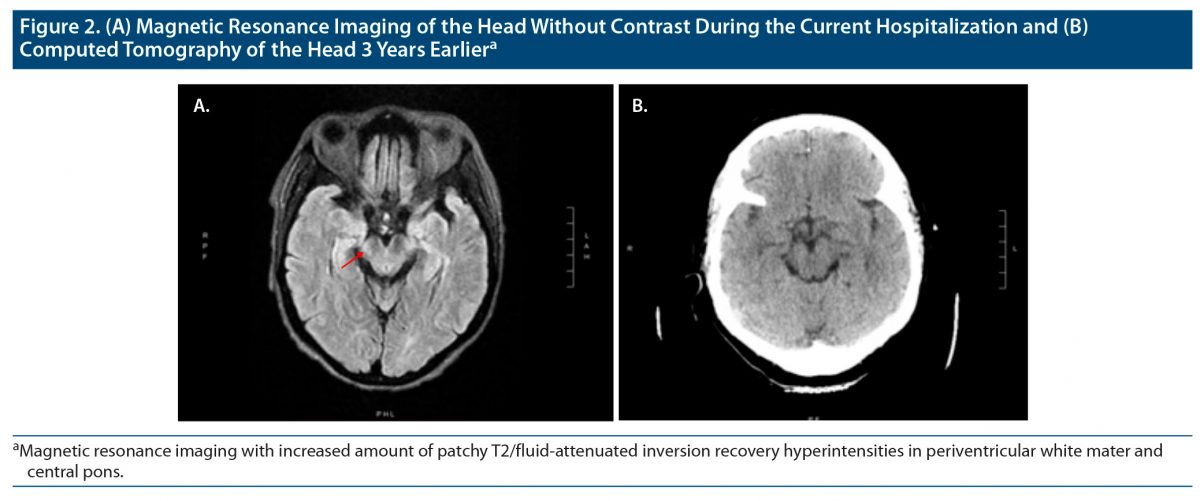
On our evaluation, Ms A lacked insight into her history of SOT or psychopathology, despite reporting delusions. She denied auditory or visual hallucinations, depressed or elated mood, and alcohol or substance misuse. She scored 43 and 29 on the Brief Psychiatric Rating Scale (BPRS)10 and Mini-Mental State Examination,11 respectively. Magnetic resonance imaging (MRI) of the brain demonstrated no acute brain abnormalities but increased amount of T2/fluid-attenuated inversion recovery (FLAIR) hyperintense signal abnormalities in the bilateral periventricular to deep hemispheric white matter and increased amount of patchy T2/flair hyperintensities in the central pons (Figure 2). There was no evidence of opportunistic infections by serum or cerebrospinal fluid examination.
On day 1 of treatment, Ms A began intravenous haloperidol titrated to 5 mg 2 times/d over 5 days. After 3 weeks of taking haloperidol, her delusions mildly attenuated, with a BPRS score of 39. At this time, intravenous haloperidol was transitioned to oral haloperidol 5 mg 2 times/d. After an additional 2 weeks of oral haloperidol, her BPRS score was 35. She was discharged on her home regimen, including haloperidol.
On monthly follow-up for 2 consecutive months, Ms A’s insight and judgment returned to her pre–SARS-CoV-2 infection level, and her final BPRS score was 18.
While initially posited as a respiratory illness, COVID-19 has demonstrated its ability to affect multiple organ systems, including the central nervous system. Potential mechanisms contributing to the pathophysiology of post/acute COVID-19 psychosis include (1) virus-specific pathophysiologic changes, including augmentation of angiotensin II signaling and prothrombotic pathways—the latter could result in microvascular ischemia and injury12 (see Figure 1); (2) immunologic aberrations and inflammatory damage in response to the acute infection13 (see Figure 1); and (3) psychosocial impacts of SARS-CoV-2 infection and increased risk of relapse of schizophrenia. Regardless of the exact etiology, Ms A’s delusions contributed to nonadherence of immunosuppressants and antipsychotics, leading to renal transplant rejection and prolongation of psychosis, respectively.
Ms A, as others with COVID-19, presented with psychotic symptoms.14–18 It is possible that her increasing amount of T2/FLAIR hyperintense signal abnormalities in bilateral periventricular to deep hemispheric white matter and pons could have precipitated her psychotic phenomenology. For instance, it has been shown that white matter integrity is disrupted in schizophrenia.19 Additionally, in metachromatic leukodystrophy, a rare autosomal recessive disorder wherein normal myelin integrity is interrupted, the progressive demyelination of periventricular white matter has been proposed to cause overt psychotic symptoms.20 Regardless, our case provides further evidence for the leading hypotheses of SARS-CoV-2–induced psychosis. Nonetheless, further studies are warranted to better understand both the pathophysiology and treatment of psychosis due to SARS-CoV-2 infection.
Received: September 7, 2021.
Published online: January 13, 2022.
Potential conflicts of interest: Dr Spiegel serves on the speakers’ bureaus for Allergen, Alkermers, Otsuka, and Intra-Cellular Therapeutics. Drs Ali, Dao, Aidukaitis, Agrawal, Bryant, and Wu report no conflicts of interest related to the subject of this report.
Funding/support: None.
Patient consent: The patient provided verbal consent to publish this case report, and the information has been de-identified to protect anonymity.
Author Affiliations

- Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
- Corresponding author: David R. Spiegel, MD, Eastern Virginia Medical School, Department of Psychiatry and Behavioral Sciences, 825 Fairfax Ave, Norfolk, VA 23507 ([email protected]).
- Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
- Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
- Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
- Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
- Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
- Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, Virginia
References (20)
- Barlati S, Nibbio G, Vita A. Schizophrenia during the COVID-19 pandemic. Curr Opin Psychiatry. 2021;34(3):203–210. PubMed CrossRef
- Toapanta N, Torres IB, Sellarés J, et al. Kidney transplantation and COVID-19 renal and patient prognosis. Clin Kidney J. 2021;14(suppl 1):i21–i29. PubMed CrossRef
- Baller EB, Hogan CS, Fusunyan MA, et al. Neurocovid: pharmacological recommendations for delirium associated with COVID-19. Psychosomatics. 2020;61(6):585–596. PubMed CrossRef
- Kozloff N, Mulsant BH, Stergiopoulos V, et al. The COVID-19 global pandemic: implications for people with schizophrenia and related disorders. Schizophr Bull. 2020;46(4):752–757. PubMed CrossRef
- Ferrando SJ, Klepacz L, Lynch S, et al. COVID-19 psychosis: a potential new neuropsychiatric condition triggered by novel coronavirus infection and the inflammatory response? Psychosomatics. 2020;61(5):551–555. PubMed CrossRef
- Ponti G, Maccaferri M, Ruini C, et al. Biomarkers associated with COVID-19 disease progression. Crit Rev Clin Lab Sci. 2020;57(6):389–399. PubMed CrossRef
- Egbert AR, Cankurtaran S, Karpiak S. Brain abnormalities in COVID-19 acute/subacute phase: a rapid systematic review. Brain Behav Immun. 2020;89:543–554. PubMed CrossRef
- Civan Kahve A, Kaya H, Darben Y, et al. From predictions to evidence: treatment compliance, disease progression and social compliance of patients with schizophrenia in the COVID-19 pandemic. Perspect Psychiatr Care. 2021;57(4):1991–1998. PubMed
- Abu Jawdeh BG. COVID-19 in kidney transplantation: outcomes, immunosuppression management, and operational challenges. Adv Chronic Kidney Dis. 2020;27(5):383–389. PubMed CrossRef
- Overall JE, Gorham DR. The Brief Psychiatric Rating Scale. Psychol Rep. 1962;10(3):799–812. CrossRef
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. PubMed CrossRef
- Ali MAM, Spinler SA. COVID-19 and thrombosis: from bench to bedside. Trends Cardiovasc Med. 2021;31(3):143–160. PubMed CrossRef
- Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601–615. PubMed CrossRef
- Huarcaya-Victoria J, Meneses-Saco A, Luna-Cuadros MA. Psychotic symptoms in COVID-19 infection: a case series from Lima, Peru. Psychiatry Res. 2020;293:113378. PubMed CrossRef
- Rentero D, Juanes A, Losada CP, et al. New-onset psychosis in COVID-19 pandemic: a case series in Madrid. Psychiatry Res. 2020;290:113097. PubMed CrossRef
- Smith CM, Komisar JR, Mourad A, et al. COVID-19–associated brief psychotic disorder. BMJ Case Rep. 2020;13(8):e236940. PubMed CrossRef
- Kozato N, Mishra M, Firdosi M. New-onset psychosis due to COVID-19. BMJ Case Rep. 2021;14(4):e242538. PubMed CrossRef
- Chacko M, Job A, Caston F 3rd, et al. COVID-19–induced psychosis and suicidal behavior: case report. SN Compr Clin Med. 2020;26:1–5. PubMed
- Ehrlich S, Geisler D, Yendiki A, et al. Associations of white matter integrity and cortical thickness in patients with schizophrenia and healthy controls. Schizophr Bull. 2014;40(3):665–674. PubMed CrossRef
- Mighdoll MI, Tao R, Kleinman JE, et al. Myelin, myelin-related disorders, and psychosis. Schizophr Res. 2015;161(1):85–93. PubMed CrossRef
Enjoy free PDF downloads as part of your membership!
![]() Save
Save
![]() Share
Share
![]() Cite
Cite



