ABSTRACT
Objective: Psychogenic purpura is a rare psychocutaneous entity characterized by painful atraumatic, ecchymotic, and purpuric lesions that commonly occur in young women. The objective of this study is to describe the clinical presentation, psychiatric profile, and response to therapy (pharmacologic and psychotherapeutic) in patients with psychogenic purpura.
Methods: Twenty-three patients, referred from various clinical departments with unexplained purpura or ecchymotic lesions, were assessed in the department of psychiatry of a tertiary care institute in eastern India over a period of 3 years (May 1, 2017, to April 30, 2020). Relevant systemic evaluation and routine biochemical and laboratory tests including complete blood count, bleeding time, clotting time, prothrombin time, coagulation profile, and platelet function test were conducted for all patients to rule out an underlying organic cause. Associated psychiatric comorbidities were diagnosed as per the International Classification of Diseases, 10th edition. All patients who were eventually diagnosed with psychogenic purpura received appropriate treatment (pharmacologic and psychotherapy) and were followed up for 1 year.
Results: Seven female patients (age range, 14–70 years, mean age = 30.28 ± 17.42 years) were diagnosed with psychogenic purpura. All patients had significant stressors prior to the appearance of lesions. Facial involvement was reported in 2 patients (28.6%). Multiple sites were affected in 4 patients (57.1%). The underlying psychiatric conditions diagnosed were depressive disorder (42.9%), generalized anxiety disorder (28.6%), dissociative convulsion disorder (14.3%), and panic disorder (14.3%). Associated personality disorder was noted in 2 patients (28.6%). All patients were started on selective serotonin reuptake inhibitors and concurrent psychotherapy. A short course of benzodiazepine was used in all patients and was subsequently tapered off. At 1-year follow-up, 2 patients reported recurrences, while others continued to do well with no similar episodes.
Conclusions: Appropriate psychiatric evaluation and necessary intervention in patients with psychogenic purpura lead to improved patient outcomes.
Prim Care Companion CNS Disord 2021;23(4):20m02870
To cite: Priyam P, Mandal US, Sil A. Psychiatric profile and response to combined pharmacologic and psychotherapeutic treatment in psychogenic purpura. Prim Care Companion CNS Disord. 2021;23(4):20m02870.
To share: https://doi.org/10.4088/PCC.20m02870
© Copyright 2021 Physicians Postgraduate Press, Inc.
aDepartment of Psychiatry, RG Kar Medical College and Hospital, Kolkata, West Bengal, India
bDepartment of Dermatology, Venereology, and Leprosy, RG Kar Medical College and Hospital, Kolkata, West Bengal, India
*Corresponding author: Abheek Sil, MBBS, Department of Dermatology, Venereology, and Leprosy, RG Kar Medical College and Hospital, 1, Khudiram Bose Sarani, Kolkata 700004, West Bengal, India ([email protected]).
Psychogenic purpura, previously referred to as Gardner-Diamond syndrome, is an extremely rare autoimmune vasculopathy characterized by recurrent atraumatic, painful, ecchymotic lesions. In their landmark publication in 1955, Gardner and Diamond1 suggested for the first time a disorder associated with autosensitization of patients to their own blood. Later, the role of phosphatidylserine in the red cell membrane was confirmed as the auto-antigen.2 Disturbance in the kallikrein-kinin system leading to dysregulation in tone of venous capillaries and dysfunctional fibrin synthesis in endothelium causing defective structures of capillary walls has also been implicated in the pathogenesis.3 Researchers have tried to find a link between pathways of stress and emotion to determine how they affect the nervous, immune, and hormonal system leading to varied skin manifestations. A stress response hypothesis explains how neuropeptide signaling molecules expressed on the cell surface via release of catecholamine and glucocorticoid lead to an altered hemostasis resulting in formation of purpuric lesions.4
Psychogenic purpura is essentially a diagnosis of exclusion with no specific ancillary findings to establish the diagnosis. It has been reported to follow severe stress or may be associated with psychiatric comorbidities such as depressive, anxiety, personality, adjustment, and conversion disorders. The overall prognosis of psychogenic purpura is favorable with no reported fatal outcomes. However, stress can precipitate relapses. Therapeutic trials with different pharmacologic agents (glucocorticoids, hormonal contraceptives, intravenous immunoglobulin, antibiotics, and plasma exchange) have had variable benefit.5
After searching PubMed and MEDLINE databases, we found only a few case series4–7 in which detailed psychiatric evaluation was undertaken and therapeutic response recorded in patients with psychogenic purpura. This study aims to contribute to the existing literature on psychogenic purpura by providing an in-depth analysis of associated psychiatric morbidities and psychological traits and assessing the response to pharmacologic and psychotherapeutic treatment.
METHODS
In this descriptive case series conducted from May 1, 2017, to April 30, 2020, 23 patients with purpura (referred from various clinical departments) attending the department of psychiatry of a tertiary care institute of eastern India were evaluated, considering the possible diagnosis of psychogenic purpura. Relevant systemic evaluations and biochemical and laboratory tests, including complete blood count, bleeding time, clotting time, prothrombin time, coagulation profile, and platelet function test, were performed to identify any underlying organic cause. Routine psychiatric workup was also conducted. The possibility of factitious purpura (induced by self or by proxy) was considered in all cases and ruled out by detailed interview of patients and relatives. Those refusing to consent for psychiatric evaluation or having an underlying organic pathology that could explain the purpura were excluded. Sixteen patients were eventually diagnosed with an underlying systemic or hematologic illness and thereby excluded. Further psychiatric profiling was done for the remaining 7 patients. The relevant data for the study were collected using a semistructured proforma for sociodemographic and clinical details. Statistical analysis was carried out using MS Excel software. Written informed consent was taken from all participating patients and their guardians (if applicable). The personal information of all patients was kept confidential, and anonymity was maintained. All patients received appropriated interventions and were followed up for 1 year.
Diagnostic Tools
The International Classification of Diseases, 10th edition (ICD-10) was used for diagnosing associated psychiatric comorbidities and their severity assessment. The Binet Kamat Test8 was used for assessment of intelligence quotient (for the purpose of standardization, we report prorated IQ). Temperament was assessed using the Junior Temperament Character Inventory.9 The International Personality Disorder Examination (IPDE)10 was utilized to assess personality disorders categorized in the ICD-10. This measure was chosen as it was compatible with the diagnosis of personality disorders in the ICD-10. A qualitative analysis of the items on the IPDE was performed to determine personality traits for the patients who did not meet the criteria for a personality disorder.
RESULTS
Demography
Seven patients, all female, were diagnosed with psychogenic purpura. The age of the patients ranged between 14 and 70 years (mean age of 30.28 ± 17.42 years).
Clinical Findings
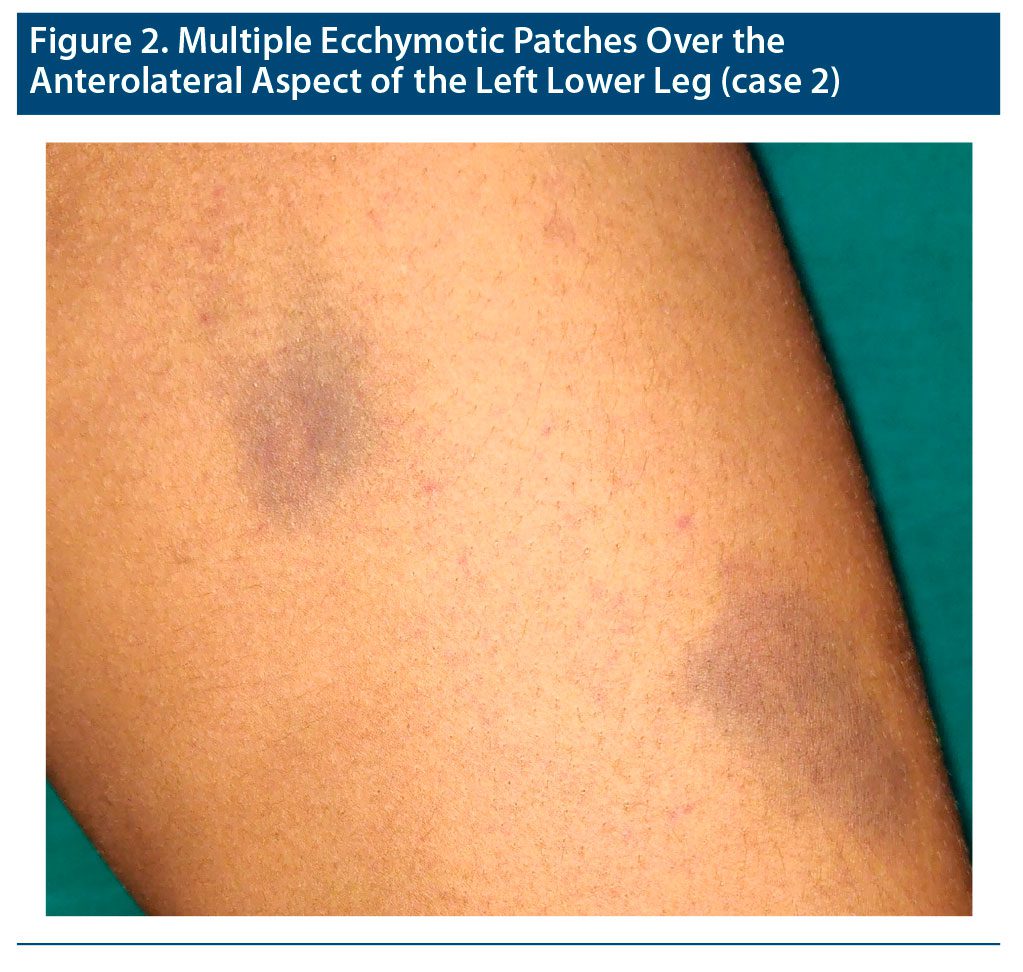
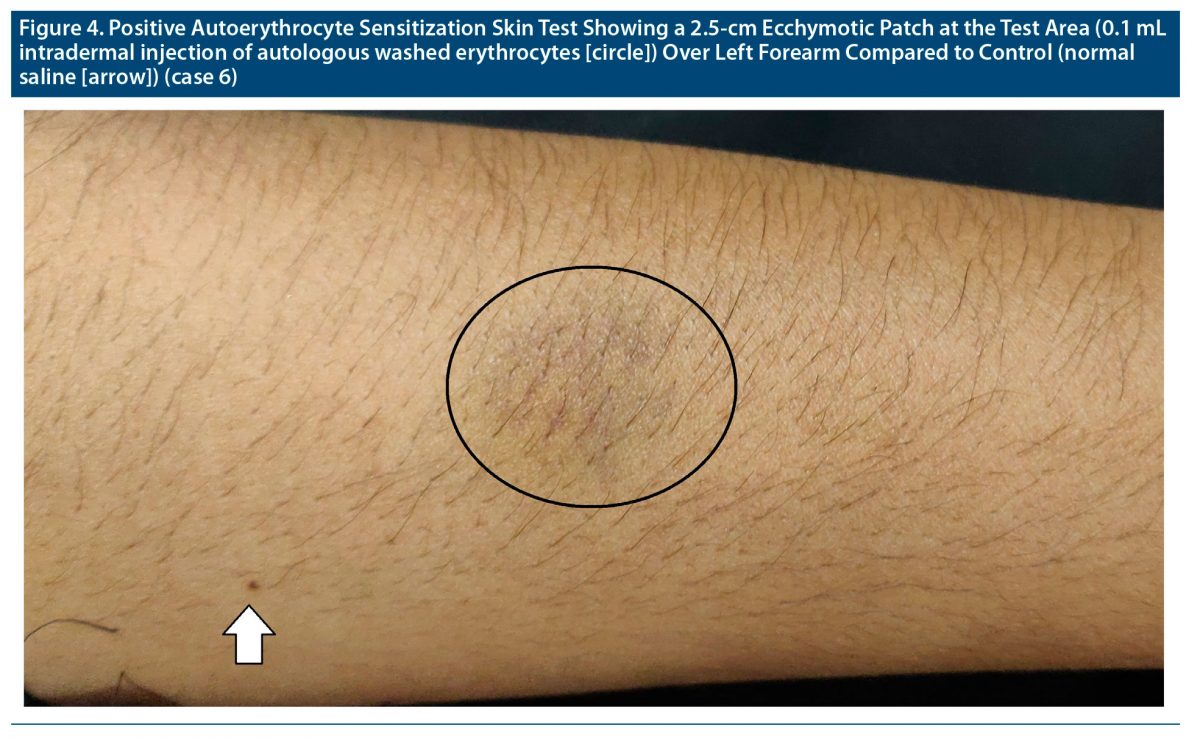
None of the patients were taking any other medications or using copper-containing contraceptive devices. No systemic manifestations or menstrual exacerbation of symptoms were reported. Systemic evaluation and relevant laboratory investigations (to rule out any systemic or hematologic abnormalities) in all cases were noncontributory. The most common site involved was the lower limbs (thigh). Facial involvement was reported by 2 patients (28.6%). All but 1 patient reported multiple lesions. Multiple sites were affected in 4 patients (57.1%) (Figure 1, Figure 2, and Figure 3). Five of 7 patients (71.4%) reported painful purpura. Six patients (85.7%) had reported multiple similar episodes in the past. Autoerythrocyte sensitization skin test was positive in 1 patient (14.3%) (Figure 4). All of the patients recalled facing significant stressors before the occurrence of purpura.


Psychiatric Comorbidities
Three patients (42.9%) had an underlying depressive disorder, 2 (28.6%) had generalized anxiety disorder, and 1 each had dissociative convulsion disorder (14.3%) and panic disorder (14.3%). Cluster C traits (dependent, avoidant) were the most common finding in the personality assessment. Two patients (28.6%) had an associated personality disorder (borderline personality and anankastic personality disorder). Cluster B (passive-aggressive, histrionic) traits were noted in 1 patient (14.3%).
Response to Combined Pharmacologic and Psychotherapeutic Intervention
The patients were started on selective serotonin reuptake inhibitors (SSRIs) and concurrent psychotherapy. A short course of benzodiazepine was used in all cases and was subsequently tapered off. During the 1-year follow-up, 2 patients (28.6%) reported recurrence, while others continued to do well. The psychiatric profile and treatment details of the patients are provided in Table 1.
DISCUSSION
Psychogenic purpura is a rare psychocutaneous disorder characterized by development of painful atraumatic ecchymosis and purpura. It can occur at any age but is most commonly seen in young women. This condition has been less commonly reported in men and adolescents. Limbs are the predominantly affected site. Rarely, multiple sites may be involved.11,12 All patients in our study were female. The unusual findings include presentation of patients with a wide age range (between 14 and 70 years) and multiple site involvement. Noteworthy was the occurrence of facial lesions in adolescent females.
The association of psychogenic purpura with psychological disturbances is quite variable. In a study5 of 200 patients with psychogenic purpura, 181 were female. Of these patients, 99 had psychiatric disorders: 48.4% had depression, 26.3% had personality disorder, and 7% presented with anxiety. Adjustment disorder and conversion disorder were reported in 2 cases each, and bipolar disorder was diagnosed in 1 case. However, the classification system used for psychiatric diagnosis was not commented on. Also, there was no specification of associated symptom severity in the patients described.5
Patients also report a host of long-standing somatic symptoms such as fatigue, weakness, pain at various sites, and gastrointestinal and urogenital disturbances that may be exacerbated with the purpuric episodes, making somatoform disorder and hypochondriasis other probable associations. Sexual problems such as dyspareunia and vaginismus may coexist.3,13 It is also proposed that purpura is a conversion symptom in response to underlying stress, as in a few cases such episodes are precipitated only by stressors and no other symptoms or organic cause is found. Although the probability of a factitious disorder cannot be denied, the appearance of new lesions on autologous washed cells at unreachable sites and under casts strongly supports the diagnosis of conversion symptoms.14 However, the utility of the autoerythrocyte sensitization skin test remains controversial due to the lack to standardization and variability in interpretation.5,12 In our study, the most common diagnosis was depressive disorder followed by anxiety disorder. One patient was diagnosed with dissociative convulsion disorder.
Some patients, who do not meet the full criteria of a psychiatric disorder present with isolated but significant psychological issues such as difficulty with interpersonal relationships, dysfunctional families, irritability, adjustment problems, and inability to tolerate hostile situations. Passive-aggressive, histrionic, borderline, and self-defeating personality traits are common in such patients.3,12 Interestingly, contrary to available literature, cluster C traits (dependent, avoidant) were more prevalent in our patients instead of cluster B traits (passive-aggressive, histrionic). Two of our patients met criteria for personality disorder.
Psychogenic purpura generally resolves without grave consequences. However, repeated relapses are often a challenge for the clinician to manage and a source of embarrassment for the patient.15 SSRIs, which have antihistaminic, anticholinergic, and serotonin-blocking properties, can lead to symptomatic improvement.16 Remission of psychogenic purpura is often concurrent with the successful management of the underlying psychiatric condition. Thus, psychotherapy has an equally important role in the management of predisposing and perpetuating conditions.17,18 Timely intervention can help curtail further episodes and avoid unnecessary investigations. All patients in this study were treated with SSRIs, a short course of benzodiazepine, and concurrent psychotherapy. A recurrence rate of 46.4% is reported in the literature.5 During the 1-year follow-up, only 2 of 7 patients (28.5%) in our study reported recurrence of purpura. Both of these patients were taking medication but had not undergone psychotherapy and had continuing stressors. Limitations of our study include a small sample size and absence of male subjects.
CONCLUSION
This study to the best of our knowledge represents the largest cohort of psychogenic purpura patients from Asia that details their underlying psychiatric comorbidities and response to treatment (pharmacotherapy and psychotherapy). As the cutaneous lesions in psychogenic purpura are distinctly visible, the burden of diagnosis often rests with a dermatologist or physician (after excluding any obvious clinical or laboratory indicator of blood dyscrasias). However, the underlying disorder may go unnoticed due to lack of liaison with psychiatric facilities. This study is an attempt to draw attention to this underrecognized disease, as it can be recurrent and fairly perturbing for the patient. An increased awareness about this psychocutaneous disorder and liaison approach to treatment will lead to improved patient outcomes.
Submitted: November 17, 2020; accepted February 3, 2021.
Published online: August 5, 2021.
Potential conflicts of interest: None.
Funding/support: None.
Patient consent: Written consent was obtained from all patients/guardians for publication of the photographs.
Clinical points
- Recurrent ecchymotic lesions with no identifiable bleeding diathesis should raise suspicion for psychogenic purpura.
- All patients with psychogenic purpura should undergo a thorough psychiatric evaluation to identify any associated psychiatric ailments.
Author Affiliations

- Department of Psychiatry, RG Kar Medical College and Hospital, Kolkata, West Bengal, India
- Department of Psychiatry, RG Kar Medical College and Hospital, Kolkata, West Bengal, India
- Department of Dermatology, Venereology, and Leprosy, RG Kar Medical College and Hospital, Kolkata, West Bengal, India
- Corresponding author: Abheek Sil, MBBS, Department of Dermatology, Venereology, and Leprosy, RG Kar Medical College and Hospital, Kolkata, West Bengal, India, 1, Khudiram Bose Sarani, Kolkata 700004, West Bengal, India ([email protected]).
References (18)
- Gardner FH, Diamond LK. Autoerythrocyte sensitization; a form of purpura producing painful bruising following autosensitization to red blood cells in certain women. Blood. 1955;10(7):675–690. PubMed CrossRef
- Groch GS, Finch SC, Rogoway W, et al. Studies in the pathogenesis of autoerythrocyte sensitization syndrome. Blood. 1966;28(1):19–33. PubMed CrossRef
- Jafferany M, Bhattacharya G. Psychogenic purpura (Gardner-Diamond syndrome). Prim Care Companion CNS Disord. 2015;17(1):14br01697. PubMed
- Tainwala RR, Phiske M, Raghuwanshi A, et al. Perplexing purpura in two females: rare case of autoerythrocyte sensitization syndrome. Indian Dermatol Online J. 2013;4(4):305–308. PubMed CrossRef
- Sridharan M, Ali U, Hook CC, et al. The Mayo Clinic experience with psychogenic purpura (Gardner-Diamond syndrome). Am J Med Sci. 2019;357(5):411–420. PubMed CrossRef
- Thokchom NS, Pradeepa D, Hafi NAB, et al. Clinical spectrum of autoerythrocyte sensitization syndrome: a series of five cases. Indian Dermatol Online J. 2018;9(2):110–113. PubMed CrossRef
- Ratnoff OD. Psychogenic purpura (autoerythrocyte sensitization): an unsolved dilemma. Am J Med. 1989;87(3N):16N–21N. PubMed
- Roopesh BN, Kumble CN, Kamat B. Test for intelligence: issues with scoring and interpretation. Indian J Ment Health. 2016;3:504–505.
- Lyoo IK, Han CH, Lee SJ, et al. The reliability and validity of the Junior Temperament and Character Inventory. Compr Psychiatry. 2004;45(2):121–128. PubMed CrossRef
- Loranger AW, Sartorius N, Andreoli A, et al. The International Personality Disorder Examination. The World Health Organization/Alcohol, Drug Abuse, and Mental Health Administration international pilot study of personality disorders. Arch Gen Psychiatry. 1994;51(3):215–224. PubMed CrossRef
- Henneton P, Frank M, Litvinova E, et al. Gardner-Diamond syndrome in a young man: a case report and literature review [in French]. Rev Med Interne. 2017;38(9):623–627. PubMed CrossRef
- Ivanov OL, Lvov AN, Michenko AV, et al. Autoerythrocyte sensitization syndrome (Gardner-Diamond syndrome): review of the literature. J Eur Acad Dermatol Venereol. 2009;23(5):499–504. PubMed CrossRef
- Ozyildirim I, Yücel B, Aktan M. Psychogenic purpura with hematuria and sexual pain disorder: a case report [in Turkish]. Turk Psikiyatr Derg. 2010;21(1):85–89. PubMed
- Stocker WW, McIntyre OR, Clendenning WE. Psychogenic purpura. Arch Dermatol. 1977;113(5):606–609. PubMed CrossRef
- Meeder R, Bannister S. Gardner-Diamond syndrome: difficulties in the management of patients with unexplained medical symptoms. Paediatr Child Health. 2006;11(7):416–419. PubMed CrossRef
- Sawant NS, Singh DA. Antidepressant-induced remission of Gardner Diamond syndrome. Indian J Psychol Med. 2012;34(4):388–390. PubMed CrossRef
- Vivekanandh K, Dash G, Mohanty P. Gardner Diamond syndrome: a psychogenic purpura. Indian Dermatol Online J. 2017;8(6):521–522. PubMed CrossRef
- Okur M, Turan H, Ozkan A, et al. An extremely rare cause of bruising in children: autoerythrocyte sensitization syndrome. Turk J Haematol. 2012;29(2):201–203. PubMed CrossRef
Enjoy free PDF downloads as part of your membership!
![]() Save
Save
![]() Share
Share
![]() Cite
Cite

