Abstract
Objective: To review the literature on the neurobiological mechanisms of obsessive-compulsive symptoms (OCS) in people with dementia.
Data Sources: MEDLINE/PubMed, CENTRAL, and PsycNet databases were searched from inception to March 2023.
Study Selection: Original studies of any methodology with newly published data on the neurobiological underpinnings of OCS in patients with dementia, regardless of patient age or comorbidity and publication year, were included. The following search terms were used: (Obses* OR compul* OR OCD) AND (cognitive de* OR cognitive dysfunction OR cognitive disfunction OR dementia).
Data Extraction: Individual study data were extracted onto a piloted extractions sheet.
Results: Patients with dementia and OCS were reported to have atrophy and hypoperfusion of frontal, temporal, striatal, and limbic structures. Serotonergic agents may be efficacious in reducing OCS. One randomized controlled trial of paroxetine in behavioral symptoms of dementia did not show efficacy. Evidence of dopaminergic dysfunction is too sparse to draw conclusions. Microglia dysfunction mediates obsessive-compulsive–like symptoms. Mutations of microtubule-associated protein τ may increase the risk of OCS. Cognitive self-consciousness and obsessive-compulsive–related cognitions may mediate OCS in old age. Dysfunction of the processing of one class of stimuli may increase the salience of other classes of stimuli, leading to OCS.
Conclusions: Frontal lobe hypometabolism and temporal lobe atrophy and hypometabolism are unexpected given previous research in obsessive compulsive disorder. Serotonergic agents have encouraging efficacy in case reports but require more specific research.
Prim Care Companion CNS Disord 2024;26(3):23r03689
Author affiliations are listed at the end of this article.
Dementia is a chronic acquired loss of cognitive abilities in at least 1 domain caused by brain disease or injury with impairment in functioning.1 Behavioral and psychological symptoms of dementia are a feature of all types of dementia and contribute to worse outcomes.2 Obsessive-compulsive symptoms (OCS) are described in 36% of patients with dementia3 and also in other neurological diseases.4 Obsessions are repetitive, unwanted, and intrusive thoughts, images, impulses, or urges commonly associated with anxiety. Compulsions are repetitive behaviors or mental acts performed in response to the obsessions that temporarily reduce the anxiety and are seen as excessive or unreasonable.5 In dementia, OCS may occur comorbid with other repetitive behavioral symptoms, such as perseveration and stereotypies, from which they are difficult to distinguish. People with obsessive-compulsive disorder (OCD) are usually able to describe the subjective aspect of compulsions, eg, an attempt to reduce distress induced by obsessions; however, in people with dementia, it may be difficult to ascertain if obsessions are absent or if they cannot be described due to impairment in cognition. Also, in people with dementia, anxiety may be less frequent, insight is usually reduced, and behaviors may have utilization characteristics.6 The objective of this scoping review was to systematically gather all literature on neurobiological mechanisms of OCS in dementia, which may shed light on the similarities and differences between OCS in dementia and in OCD.
METHODS
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta Analyses extension for scoping reviews.7,8 It was not registered in PROSPERO, as this platform does not register scoping reviews. We included original studies of any methodology with newly published data on the neurobiological underpinnings of OCS in patients with dementia. Studies were accepted regardless of patient age, comorbidity, dementia severity, and publication year. Studies in English, Portuguese, Spanish, and French were included. It was decided that patient age and dementia severity should not be inclusion criteria since we were not interested in dementia of any particular age at onset and because the point of scoping reviews is to obtain a wide view of literature. We excluded publications on other diagnoses, dementia with no information about OCS, other psychiatric symptoms, and neuropsychological evaluation with no information about dementia, as well as publications with no new information. We searched MEDLINE/ PubMed, CENTRAL, and PsycNet databases from inception to March 2023. Reference lists were cross checked for additional references. The following search terms were used: (Obses* OR compul* OR OCD) AND (cognitive de* OR cognitive dysfunction OR cognitive disfunction OR dementia). Two reviewers independently screened titles, abstracts, and full texts. Disagreements were solved by consensus. One reviewer extracted individual study data into a piloted extractions sheet. Another reviewer confirmed the extracted data. We collected the following data items, when available: author, year of publication, study design, duration and country, inclusion and exclusion criteria, dementia diagnosis, and any insight into the neurobiology of OCS in dementia. Due to the scoping nature of this review, the included articles had varying methodologies. For this reason, a comparative critical appraisal of evidence was impossible. All authors contributed in reviewing the extracted data.
RESULTS
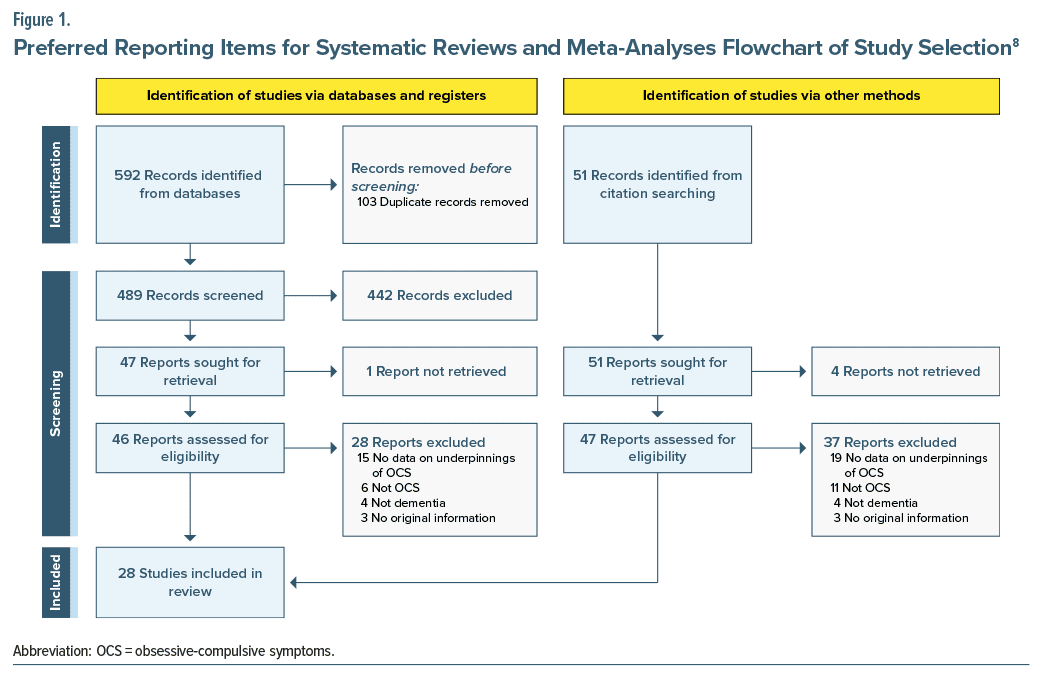
Of the 646 articles screened, 98 were accepted for full-text assessment. Of these, 28 articles had information about the neurobiological underpinnings of OCS in dementia (Figure 1). We sent emails to the authors of 5 studies requesting articles that we were unable to find in online databases and received no replies over 30 days, which led to the automatic exclusion of those references. No study was excluded due to language.
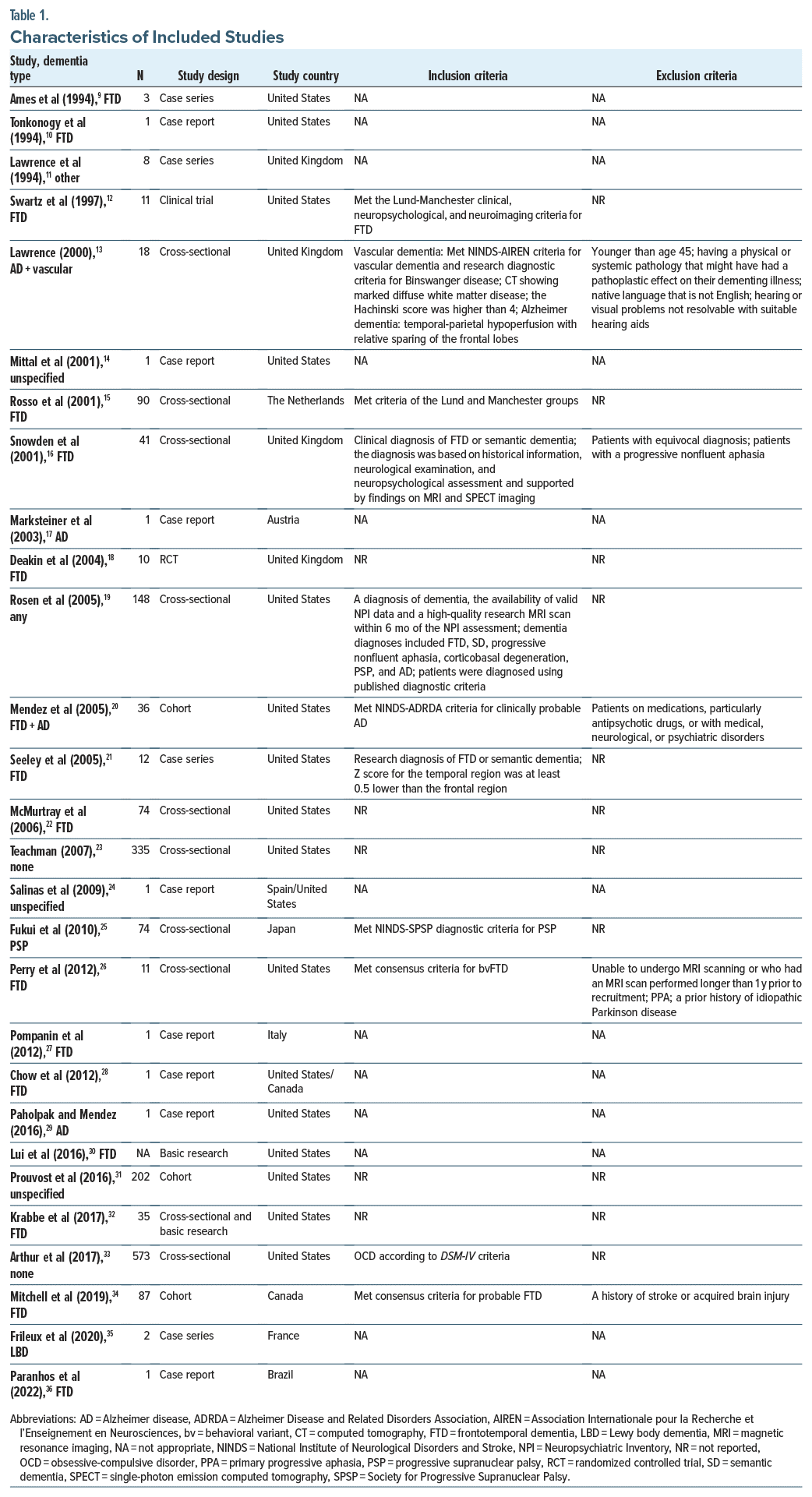
 For data on the included studies, see Table 1. Most studies (10) had a cross-sectional design.13,15,16,19,22,23,25,26,32,33 A significant proportion were case reports (8)10,14,17,24,27–29,36 or case series (4).9,11,21,35 There were also cohort studies (3)20,31,34 and clinical trials (2).12,18 We also included basic research studies (2),30,32 1 of which also described a cross-sectional assessment of patients.32 Among the 28 included studies, there were 30 cohorts: 1 included 2 cohorts of Alzheimer disease (AD) and vascular dementia14 and another included 2 cohorts of frontotemporal dementia (FTD) and AD.20 Most were cohorts of people with FTD, some FTD subtype, or Pick disease (16).9,10,12,15,16,18,20–22,26–28,30,32,34,36 Other relevant diagnoses were AD (4)13,17,20,29 and nonspecified dementia (3).14,24,31 One study included patients with focal cortical degeneration in several locations,11 1 included patients with vascular dementia,13 1 included patients with Lewy body dementia (LBD),35 1 included patients with progressive supranuclear palsy (PSP),25 and 1 included patients with dementia of any type.19 Two studies did not enroll patients with dementia23,33; however, we felt that they were valuable for our objective. One of those studies assessed cognitive concerns and OCS in younger and older-aged people23 and another searched for C9orf72 mutations in people with OCD diagnosis.33
For data on the included studies, see Table 1. Most studies (10) had a cross-sectional design.13,15,16,19,22,23,25,26,32,33 A significant proportion were case reports (8)10,14,17,24,27–29,36 or case series (4).9,11,21,35 There were also cohort studies (3)20,31,34 and clinical trials (2).12,18 We also included basic research studies (2),30,32 1 of which also described a cross-sectional assessment of patients.32 Among the 28 included studies, there were 30 cohorts: 1 included 2 cohorts of Alzheimer disease (AD) and vascular dementia14 and another included 2 cohorts of frontotemporal dementia (FTD) and AD.20 Most were cohorts of people with FTD, some FTD subtype, or Pick disease (16).9,10,12,15,16,18,20–22,26–28,30,32,34,36 Other relevant diagnoses were AD (4)13,17,20,29 and nonspecified dementia (3).14,24,31 One study included patients with focal cortical degeneration in several locations,11 1 included patients with vascular dementia,13 1 included patients with Lewy body dementia (LBD),35 1 included patients with progressive supranuclear palsy (PSP),25 and 1 included patients with dementia of any type.19 Two studies did not enroll patients with dementia23,33; however, we felt that they were valuable for our objective. One of those studies assessed cognitive concerns and OCS in younger and older-aged people23 and another searched for C9orf72 mutations in people with OCD diagnosis.33
Dysfunction of Frontal Structures
Frontal structures, particularly the orbitofrontal cortex (OFC), have been widely implicated in OCD.37 People with OCD present with hypermetabolism and reduced volume in the OFC in positron emission tomography (PET) and magnetic resonance imaging (MRI) studies.38 In all, the evidence that we review here may support that people who present with OCS have frontal, particularly OFC, dysfunction. However, while reduced frontal or OFC volume is described in both disorders, dementia seems to present with hypometabolism in frontal structures (see below), unlike OCD. Patients with vascular dementia, when compared with patients with AD, were shown to have more OCS and more marked leukoaraiosis in periventricular and frontal white matter; however, there was no comparison of leukoaraiosis between patients with and without OCS.13 In 2 single-photon emission computed tomography (SPECT) studies, OCS were correlated with right frontal hypoperfusion in 74 people with FTD22 and OFC hypoperfusion in 74 people with PSP.25 In a PET study of 10 patients with focal cortical atrophy, 8 had OCS, and of those, 6 had hypometabolism in left frontal or frontotemporal regions.11 The 2 patients in this study who did not have OCS had posterior cortical atrophy. In 20 symptomatic carriers of progranulin mutations, compared to 42 controls, voxel-based morphometry analyses of structural MRI scans revealed that carriers had extensive frontotemporal atrophy, and among carriers, over half had repetitive and compulsive behaviors compared to none of the controls. However, there were no comparisons of volume in patients with and without OCS.32 On the other hand, in a case report of a patient with Pick disease, OCS were more prominent early in the development of the illness, when only caudate atrophy was noted. Later, as frontal atrophy developed, OCS abated and eventually disappeared.10
Dysfunction of Striatal Areas
Dysfunction in the frontal cortico-striato-thalamo cortical (CSTC) pathway has been described in relation to OCD and OCS; in particular, there may be increased gray area volume in striatal areas,38 as well as evidence of efficacy of DBS in CSTC sites for OCD.39 Several of the included studies suggest that damage to the structures involved in this pathway by disease mechanisms that also cause dementia may present in patients with late onset OCS, however, in the opposite direction. In 74 people with PSP, OCS were correlated but not statistically significantly with hypoperfusion in the thalamus and caudate in SPECT.25 In 11 patients with behavioral variant FTD (bvFTD), compared with healthy controls, the OCS correlated with gray matter loss in the bilateral globus pallidus and left putamen.26 In 20 symptomatic carriers of progranulin mutations (over half of which with OCS), there was more significant striatum atrophy compared to controls. In a case series of frontal lobe degeneration, one of the patients presented with OCS and caudate hypoperfusion in SPECT.9 In another case report of a patient with OCD and early-onset dementia, severe caudate degeneration was described. A case series24 describes 3 older individuals who experienced OCD reactivation after years without symptoms: after cerebrovascular lesions or hypoxic brain damage involving basal ganglia and internal capsule in 1 patient, frontal lobe and left caudate in another patient, and left thalamus in a third patient. Krabbe and colleagues32 reported that progranulin deficient mice (that have excessive grooming OCD-like behaviors) presented with increased excitability of nucleus accumbens neurons, mediated by tumor necrosis factor-α (TNF-α). On the other hand, in a study of computed tomography and MRI of 90 patients with FTD, caudate abnormalities did not seem to mediate OCS.15
Dysfunction of Temporal Structures
While the OFC, anterior cingulate cortex, and basal ganglia have been implicated in the pathophysiology of OCD,37 the temporal lobe has received much less attention. However, acquired OCD has been described in patients with temporal lobe lesions40 and temporal lobe epilepsy. Several mechanisms have been proposed,41 but there are no clear answers for this association. That said, several included studies found temporal lobe abnormalities in patients with dementia and OCS. Several FTD versus control studies correlate OCS with temporal lobe atrophy in MRI and temporal hypometabolism in SPECT or PET,15,22,26 and case reports9,27 also describe that relationship. Temporal atrophy is also a feature of a cohort of progranulin carriers, over half of which presented with OCS.32 In a comparison of patients with semantic dementia and other FTD diagnoses, both OCS and temporal atrophy and hypometabolism were more frequent in the semantic dementia cohort.16
Dysfunction of Limbic Structures
More recently, the CSTC model for OCD has been modified to also include the limbic structures (hippocampus, anterior cingulate cortex, and amygdala), all of which connected with the OFC.38 Dysfunction in these structures has been described in patients with dementia and OCS, namely, increased volume in the cingulate cortex and loss of volume in the amygdala and hippocampus. In people with probable FTD, OCS correlated with atrophy in the anterior cingulate gyrus, amygdala, and hippocampus bilaterally,34 and in a case report of semantic dementia and OCD, the authors27 describe atrophy of the amygdala and the anterior cingulate cortex as well as hypometabolism in the left cingulate cortex in PET. In a study with 148 patients that looked for correlates between behavioral disorders measured by the Neuropsychiatric Inventory (NPI) and brain volume changes (measured by voxel-based morphometry), the aberrant motor behavior item of the NPI correlated with tissue loss in the dorsal anterior cingulate cortex. However, this NPI item is not specific to compulsions and also includes other repetitive motor behaviors.19
Dysfunction of Serotonin Neurotransmission
The efficacy of drugs that bind to the serotonin transporter has been clearly established in OCD.42 However, this has scarcely translated to an unequivocal understanding of the role of serotonin in OCD.37 Similarly, there have been some reports of the efficacy of these drugs in OCS in dementia, with little understanding of their mechanism. Selective serotonin reuptake inhibitors (SSRIs) have been shown to downregulate serotonin 1D autoreceptors in the OFC in animal studies of OCD, which may tie the efficacy of these agents with correction of OFC abnormalities.38 One review of the evidence regarding neurotransmitter function in FTD reported (1) a decrease in serotonin receptors in OFC, frontal medial cortex, and cingulate cortex; (2) a decrease in binding of serotonin; and (3) neuronal loss in the raphe nuclei43; however, there is no direct evidence that connects these changes in dementia with OCS. Among the included studies, there is some tentative evidence that serotonin dysfunction may mediate OCS in people with dementia. In an 80-year-old patient with probable AD and severe OCS, there was a significant reduction in the density of serotonin transporter sites using SPECT.17 After treatment with fluoxetine, there was significant improvement in OCS and increase in density of serotonin transporter sites.17 There are several case series and case reports of SSRI use in patients with dementia that suggest an improvement in OCS.12,20,28 However, a randomized controlled trial (RCT) of paroxetine for behavioral symptoms of FTD did not show efficacy.18 Also, in a 68-year-old patient with logopenic variant primary progressive aphasia and OCD, sertraline, paroxetine, and olanzapine were not effective.36
Dysfunction of Dopamine Neurotransmission
Dopamine activity may have a role to play in OCS in dementia. In a review of the role of dopamine in the pathophysiology of OCD, the authors44 propose that ascending serotonergic projections from the raphe nuclei moderate the activity of dopaminergic CSTC frontal loops. They posit that in OCD, there is dopaminergic hyperactivity induced by serotonergic hypoactivity in these loops.44 This is in line with evidence of the efficacy of antidopaminergic agents such as quetiapine and risperidone.45 One review of the evidence regarding neurotransmitter function in FTD reported abnormalities in dopamine function in patients with FTD.43 There is scarce evidence to go by on what relates dopamine to OCS in dementia. There is 1 case report of a patient with AD and trichotillomania that showed improvement with quetiapine 150 mg; however, this dose most likely has scarce effect on dopamine function.29 Some authors describe patients with OCS and LBD (2 patients)35 and PSP (74 patients, 24% of which had OCS),25 both synucleinopathies with dopamine dysfunction; the authors propose that this may have been related to OCS. In 1 case report of semantic dementia with comorbid OCD, the patient had evidence of dopaminergic impairment in DaT Scan, and the authors27 argue that this may be related to the atypical features the patient presented, such as OCS.
Microglia Dysfunction
Two basic research studies cast light on how microglia dysfunction mediates progranulin deficiency and OCD-like grooming behavior in mice.30,32 In a study, the authors describe excessive pruning by microglia of inhibitory synapses in the ventral thalamus, mediated by complement activation. These mice then have hyperexcitability in the thalamocortical circuits and present with OCD-like grooming behaviors.30 In another study, mice presented with impaired microglia dysfunction that mediated self-grooming OCD-like behavior. Also, NF-κB–induced TNF-α activity was shown to mediate the presence of excessive grooming phenotype but did not mediate social deficits that these mice also present. These mice also presented with increased excitability of nucleus accumbens neurons, also mediated by TNF-α.32
Genetic Evidence
Some studies tried to determine if OCS in dementia could have genetic abnormalities commonly seen in FTD as a cause. Two studies30,32 found that mice with progranulin deficiency had OCD-like grooming behaviors, one of which also described that among 45 carriers of progranulin mutations, 57% had repetitive and compulsive behaviors (more so the symptomatic carriers, among whom 70% had repetitive and compulsive behaviors), compared with none of healthy controls.32 They did not, however, compare with patients with FTD without progranulin deficiency, so the relevance of the mutation is hard to infer. Another study performed genetic screening for the C9orf72 repeat expansion on 573 patients diagnosed with OCD and found that none carried the expansion.33 In 11 patients with bvFTD, 9 of which with OCS, 1 study found that the 5 patients who had microtubule-associated protein τ (MAPT) mutations were among the top 7 Yale-Brown Obsessive Compulsive Scale scores, which, after regression analysis, may have been partially driven by the MAPT mutations.26
Cognitive Models
In a review of cognitive processes of OCS in older adults, the authors46 suggested that perhaps concerns about cognitive functioning could lead to greater monitoring of thoughts, making normal intrusive thoughts more salient and activating more effortful thought control attempts; however, this hypothesis has not been adequately studied so far. There are, however, some published data that may shed light on the relationship between cognitive processes and the development of OCS in dementia. In a study31 of 99 older adults, the authors assessed whether cognitive self consciousness (a tendency to be aware of and monitor thinking) might increase reactivity to aging-related cognitive changes and mediate the relationship between cognitive functioning and OCS. They concluded that lower scores of cognitive function predicted higher cognitive self-consciousness, which in turn predicted higher OCS scores. They posit that patients with higher cognitive self-consciousness may process stimuli less efficiently and with greater reactivity to intrusive thoughts.31 In a study of 355 people,23 the authors concluded that the relationship between OCD-related dysfunctional beliefs (such as over-importance of thoughts) and OCD symptoms is partially mediated by subjective cognitive concerns. When comparing people under and over the age of 65 years, those over 65 years had greater levels of subjective cognitive concerns, but those were not more important in the link between beliefs and symptoms. So, complaints about cognitive function have an important contribution to OCD, regardless of age.23 In a study of 12 patients with predominantly temporal FTD, 11 of which had OCS, the authors propose that primary temporal pathology changes the salience of different classes of stimuli, which may lead to compulsions. In patients with right-sided temporal atrophy, there is a loss of social and visual cues, so verbal stimuli acquire salience, and the patient may develop compulsions related with those, eg, word games. Conversely, in patients with left-sided temporal atrophy, there is a loss of meaning of verbal cues, so visual cues become more salient and subject of compulsions, eg, cleaning or collecting shiny objects.21
DISCUSSION
We found that people with dementia and OCS presented with frontal and OFC atrophy and hypometabolism. Atrophy parallels the loss of volume described in OCD, but hypometabolism is not consistent with findings of OFC hypermetabolism in OCD. We found atrophy and hypoperfusion of several different striatal regions, which may not be consistent with evidence of increased striatal gray matter volume in people with OCD, and atrophy in limbic areas, which is not entirely consistent with evidence of increased volume in cingulate cortex and decreased volume in amygdala and hippocampus in people with OCD. Temporal lobe atrophy and hypometabolism were frequently described in the literature of OCS in dementia, which has not been as consistently described in OCD patients. This relationship between temporal atrophy and hypometabolism and OCS is surprising. One study15 proposes that temporal lesions disrupt the frontal CSTC circuitry involved in the suppression of compulsive thoughts and behavior, leading to increased frontal activity that would lead to OCS. This would fit with the OFC hypermetabolism evident in OCD but does not fit with frontal hypometabolism in patients with dementia and OCS. These differences may mean that pathophysiologic mechanisms of OCS in people with dementia are different from those with OCD; however, they may also mean that these behaviors are not OCS but are other types of repetitive behaviors common in dementia. Temporal changes in particular may suggest that OCS behaviors are repetitive behaviors due to memory impairment and not proper OCS.
OCS in people with dementia showed improvement with serotonergic agents in case reports and case series, but behavioral symptoms did not improve in an RCT of paroxetine. These data are too sparse to draw any conclusion. Patients with OCD also improve with serotonergic agents, but so do other behavioral and psychiatric symptoms of dementia, so response to treatment allows little clarification about the nature of symptoms. Literature on dopaminergic dysfunction in OCS in dementia is too scarce. In progranulin deficient mice, microglia dysfunction was shown to mediate OCS-like behaviors. Patients with bvFTD with MAPT mutations may have more severe OCS. Cognitive self-consciousness and OCS-related cognitions (eg, the over-importance of thoughts) may mediate OCS in old age. Dysfunction of the processing of one class of stimuli may increase the salience of other classes of stimuli, leading to OCS about these.
The most consistent findings are that OCS in dementia are related to frontal and temporal abnormalities. Less consistent are the data that relate OCS with abnormalities in various striatal regions. Other findings can at best be viewed as tentative. Most of the included cohorts (16 of 30) pertain to FTD. It is safe to argue that dysfunction in frontal and temporal regions, most prominent in FTD, contributes to the emergence of OCS, which seems to be most frequent in this type of dementia. However, if patients with other causes of dementia also have prominent dysfunction in these regions, OCS may also emerge.
It is currently unclear if predementia OCD, OCS, or obsessive-compulsive personality traits, diagnosed or otherwise, increase the risk of dementia-related OCS. Some of these data suggest that neurobiological and cognitive mechanisms may be shared in both instances. In theory, the presence of OCD, OCS, or obsessive compulsive personality traits may represent the presence of these mechanisms that, when added to dementia-related cerebral insults, reactivate or exacerbate OCS. One study did report the reactivation of previously treated OCD with the onset of dementia.24 However, more research is needed.
Limitations
We made a significant effort to include only studies that included patients with clear OCS and not only other repetitive behaviors; still, given the high frequency of other repetitive behaviors in dementia, it is difficult to be certain of the phenomenological characteristics of behaviors. This is a particularly important point for future research to focus on since different repetitive behaviors/ OCS have different neurobiology and respond differently to various interventions. While some of the included studies had controlled design and compared people with OCS with those without, or people with dementia with controls, most were case reports or case series.
Dementia is an overarching syndrome with many different causes, and mechanisms of OCS may differ among causes; it was not possible to evaluate OCS within specific diagnoses. Most of the included studies pertain to FTD, and we believe most of the results herein are driven by FTD data, despite that AD is the most frequent cause of dementia. Some of the most consistent results in the literature are that OCS in dementia are related to frontal and temporal abnormalities, particularly frequent in FTD. In most studies, OCS correlated with several different changes (eg, frontal, temporal, and basal ganglia abnormalities), rendering it impossible to tease apart which change is most related to OCS.
CONCLUSION
We found an association between frontal lobe hypometabolism and OCS, as well as temporal lobe atrophy and hypometabolism and OCS, which was unexpected given previous research in OCD. Abnormalities in these regions are most prominent in FTD, and most of the included data pertained to this diagnosis. Other findings are less consistent. Serotonergic agents have encouraging efficacy in case reports but require further research. The phenomenological distinction between OCS and other repetitive behaviors in dementia also renders further research necessary. Further research is also needed to detail what type of OCS is associated with temporal atrophy, as some OCS may be phenomenologically related to memory impairment, such as obsessions of doubt and checking compulsions.
Article Information
Published Online: June 18, 2024. https://doi.org/10.4088/PCC.23r03689
© 2024 Physicians Postgraduate Press, Inc.
Submitted: December 20, 2023; accepted February 28, 2024.
To Cite: Martinho FP, Ferreira TF, Magalhães D, et al. Obsessive-compulsive symptoms in dementia: scoping review of pathological changes.
Prim Care Companion CNS Disord. 2024;26(3):23r03689.
Author Affiliations: Psychiatry and Mental Health Department, Hospital Professor Doutor Fernando Fonseca, EPE, Lisboa, Portugal (all authors).
Corresponding Author: Psychiatry and Mental Health Department, Hospital Professor Doutor Fernando Fonseca, EPE, IC19, 2720-801, Amadora, Lisboa, Portugal ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
Previous Presentation: This work was presented as an oral communication at the 30th European Congress of Psychiatry; June 5, 2022; Budapest.
ORCID: Filipe P. Martinho: https://orcid.org/0000-0002-7703-081X
Clinical Points
- Obsessive-compulsive symptoms (OCS) were found to be associated with temporal and frontal lobe hypometabolism and temporal lobe atrophy.
- Most patients found to have OCS have frontotemporal dementia.
- Selective serotonin reuptake inhibitors may be of use in patients suffering with OCS.
Author Affiliations

- Psychiatry and Mental Health Department, Hospital Professor Doutor Fernando Fonseca, EPE, Lisboa, Portugal
- Psychiatry and Mental Health Department, Hospital Professor Doutor Fernando Fonseca, EPE, Lisboa, Portugal
- Psychiatry and Mental Health Department, Hospital Professor Doutor Fernando Fonseca, EPE, Lisboa, Portugal
- Psychiatry and Mental Health Department, Hospital Professor Doutor Fernando Fonseca, EPE, Lisboa, Portugal
- Psychiatry and Mental Health Department, Hospital Professor Doutor Fernando Fonseca, EPE, Lisboa, Portugal
References (46)
- Arvanitakis Z, Shah RC, Bennett DA. Diagnosis and management of dementia: review. Jama. 2019;322(16):1589–1599. PubMed CrossRef
- Cerejeira J, Lagarto L, Mukaetova-Ladinska EB. Behavioral and psychological symptoms of dementia. Front Neurol. 2012;3:73. PubMed
- Ferreira TF, Martinho F, Felício R, et al. Obsessive-compulsive symptoms in dementia: synthesis of a meta-analytic study. In: Poster presented at: 17th Annual Scientific Meeting – International College of Obsessive-Compulsive Spectrum Disorders. Virtual. Accessed October 1, 2021.
- Pena MC, Vale FD. Sintomas obsessivo-compulsivos nas demências. Arch Clin Psychiatry. 2010;37(3):124–130.
- Stein DJ, Costa DLC, Lochner C, et al. Obsessive–compulsive disorder. Nat Rev Dis Primers. 2019;5(1):52. PubMed CrossRef
- Ducharme S, Price BH, Larvie M, et al. Clinical approach to the differential diagnosis between behavioral variant frontotemporal dementia and primary psychiatric disorders. Am J Psychiatry. 2015;172(9):827–837. PubMed CrossRef
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. PubMed CrossRef
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. PubMed CrossRef
- Ames D, Cummings JL, Wirshing WC, et al. Repetitive and compulsive behavior in frontal lobe degenerations. J Neuropsychiatry Clin Neurosci. 1994;6(2):100–113. PubMed CrossRef
- Tonkonogy JM, Smith TW, Barreira PJ. Obsessive-compulsive disorders in Pick’s disease. J Neuropsychiatry Clin Neurosci. 1994;6(2):176–180. PubMed CrossRef
- Lawrence RM, Ronca MA, Tyrrell P, et al. Psychiatric symptoms in patients with focal cortical degeneration. Behav Neurol. 1994;7(3):153–158. PubMed CrossRef
- Swartz JR, Miller BL, Lesser IM, et al. Frontotemporal dementia: treatment response to serotonin selective reuptake inhibitors. J Clin Psychiatry. 1997;58(5):212–216. PubMed
- Lawrence RM. Is the finding of obsessional behaviour relevant to the differental diagnosis of Vascular Dementia of the Binswanger Type? Behav Neurol. 2000;12(3):149–154. PubMed CrossRef
- Mittal D, O’Jile J, Kennedy R, et al. Trichotillomania associated with dementia: a case report. Gen Hosp Psychiatry. 2001;23(3):163–165. PubMed CrossRef
- Rosso SM, Roks G, Stevens M, et al. Complex compulsive behaviour in the temporal variant of frontotemporal dementia. J Neurol. 2001;248(11):965–970. PubMed CrossRef
- Snowden JS, Bathgate D, Varma A, et al. Distinct behavioural profiles in frontotemporal dementia and semantic dementia. J Neurol Neurosurg Psychiatry. 2001;70(3):323–332. PubMed CrossRef
- Marksteiner J, Walch T, Bodner T, et al. Fluoxetine in Alzheimer’s disease with severe obsessive compulsive symptoms and a low density of serotonin transporter sites. Pharmacopsychiatry. 2003;36(5):207–209. PubMed CrossRef
- Deakin JB, Rahman S, Nestor PJ, et al. Paroxetine does not improve symptoms and impairs cognition in frontotemporal dementia: a double-blind randomized controlled trial. Psychopharmacology (Berl). 2004;172(4):400–408. PubMed CrossRef
- Rosen HJ, Allison SC, Schauer GF, et al. Neuroanatomical correlates of behavioural disorders in dementia. Brain. 2005;128(Pt 11):2612–2625. PubMed CrossRef
- Mendez MF, Shapira JS, Miller BL. Stereotypical movements and frontotemporal dementia. Mov Disord. 2005;20(6):742–745. PubMed CrossRef
- Seeley WW, Bauer AM, Miller BL, et al. The natural history of temporal variant frontotemporal dementia. Neurology. 2005;64(8):1384–1390. PubMed CrossRef
- McMurtray AM, Chen AK, Shapira JS, et al. Variations in regional SPECT hypoperfusion and clinical features in frontotemporal dementia. Neurology. 2006;66(4):517–522. PubMed CrossRef
- Teachman BA. Linking obsessional beliefs to OCD symptoms in older and younger adults. Behav Res Ther. 2007;45(7):1671–1681. PubMed CrossRef
- Salinas C, Dávila G, Berthier ML, et al. Late-life reactivation of obsessive compulsive disorder associated with lesions in prefrontal-subcortical circuits. J Neuropsychiatry Clin Neurosci. 2009;21(3):332–334. PubMed CrossRef
- Fukui T, Lee E, Hosoda H, et al. Obsessive-compulsive behavior as a symptom of dementia in progressive supranuclear palsy. Dement Geriatr Cogn Disord. 2010;30(2):179–188. PubMed CrossRef
- Perry DC, Whitwell JL, Boeve BF, et al. Voxel-based morphometry in patients with obsessive-compulsive behaviors in behavioral variant frontotemporal dementia. Eur J Neurol. 2012;19(6):911–917. PubMed CrossRef
- Pompanin S, Perini G, Toffanin T, et al. Late-onset OCD as presenting manifestation of semantic dementia. Gen Hosp Psychiatry. 2012;34(1):102.e1–102.e4. PubMed CrossRef
- Chow TW, Links KA, Masterman DL, et al. A case of semantic variant primary progressive aphasia with severe insular atrophy. Neurocase. 2012;18(6):450–456. PubMed CrossRef
- Paholpak P, Mendez MF. Trichotillomania as a manifestation of dementia. Case Rep Psychiatry. 2016;2016:9782702. PubMed CrossRef
- Lui H, Zhang J, Makinson SR, et al. Progranulin deficiency promotes circuit specific synaptic pruning by microglia via complement activation. Cell. 2016;165(4):921–935. PubMed CrossRef
- Prouvost C, Calamari JE, Woodard JL. Does cognitive self-consciousness link older adults’ cognitive functioning to obsessive-compulsive symptoms? Behav Res Ther. 2016;85:23–32. PubMed CrossRef
- Krabbe G, Minami SS, Etchegaray JI, et al. Microglial NFκB-TNFα hyperactivation induces obsessive–compulsive behavior in mouse models of progranulin-deficient frontotemporal dementia. Proc Natl Acad Sci U S A. 2017;114(19):5029–5034. PubMed CrossRef
- Arthur KC, Rivera AM, Samuels J, et al. C9orf72 hexanucleotide repeat expansions are not a common cause of obsessive-compulsive disorder. J Neurol Sci. 2017;375:71–72. PubMed CrossRef
- Mitchell E, Tavares TP, Palaniyappan L, et al. Hoarding and obsessive–compulsive behaviours in frontotemporal dementia: clinical and neuroanatomic associations. Cortex. 2019;121:443–453. PubMed CrossRef
- Frileux S, Millet B, Fossati P. Late-onset OCD as a potential harbinger of dementia with Lewy bodies: a report of two cases. Front Psychiatry. 2020;11:554. PubMed
- Paranhos T, Lucas T, de Salles A, et al. A presumptive association between obsessive compulsions and asymmetric temporal lobe atrophy: a case report. J Med Case Rep. 2022;16(1):21. PubMed
- Goodman WK, Storch EA, Sheth SA. Harmonizing the neurobiology and treatment of obsessive-compulsive disorder. Am J Psychiatry. 2021;178(1):17–29. PubMed
- Menzies L, Chamberlain SR, Laird AR, et al. Integrating evidence from neuroimaging and neuropsychological studies of obsessive-compulsive disorder: the orbitofronto-striatal model revisited. Neurosci Biobehav Rev. 2008;32(3):525–549. PubMed CrossRef
- Gadot R, Najera R, Hirani S, et al. Efficacy of deep brain stimulation for treatment resistant obsessive-compulsive disorder: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2022;93:1166–1173.
- Berthier ML, Kulisevsky J, Gironell A, et al. Obsessive-compulsive disorder associated with brain lesions: clinical phenomenology, cognitive function, and anatomic correlates. Neurology. 1996;47(2):353–361. PubMed CrossRef
- Kaplan PW. Epilepsy and obsessive-compulsive disorder. Dialogues Clin Neurosci. 2010;12(2):241–248. PubMed CrossRef
- Soomro GM, Altman DG, Rajagopal S, et al. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). Cochrane Database Syst Rev. 2008;2008(1):CD001765. PubMed CrossRef
- Huey ED, Putnam KT, Grafman J. A systematic review of neurotransmitter deficits and treatments in frontotemporal dementia. Neurology. 2006;66(1):17–22. PubMed CrossRef
- Koo MS, Kim EJ, Roh D, et al. Role of dopamine in the pathophysiology and treatment of obsessive–compulsive disorder. Expert Rev Neurother. 2010;10(2):275–290. PubMed CrossRef
- Komossa K, Depping AM, Meyer M, et al. Second-generation antipsychotics for obsessive compulsive disorder. Cochrane Database Syst Rev. 2010;(12):CD008141. PubMed CrossRef
- Calamari JE, Janeck AS, Deer TM. Cognitive processes and obsessive compulsive disorder in older adults. In: Frost RO, Steketee G, eds. Cognitive Approaches to Obsessions and Compulsions. Pergamon;2002:315–335.
Enjoy free PDF downloads as part of your membership!
![]() Save
Save
![]() Share
Share
![]() Cite
Cite