![]()
Prim Care Companion CNS Disord 2021;23(6):20cr02894
To cite: Kritzer MD, Buch K, Mukerji SS, et al. Cases of neuroinfectious disease highlighting frontotemporal neurocircuitry in cognitive and affective processing. Prim Care Companion CNS Disord. 2021;23(6):20cr02894.
To share: https://doi.org/10.4088/PCC.20cr02894
© Copyright 2021 Physicians Postgraduate Press, Inc.
aDivision of Neuropsychiatry, Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts
bDepartment of Radiology, Massachusetts General Hospital, Boston, Massachusetts
cDepartment of Neurology, Massachusetts General Hospital, Boston, Massachusetts
dDivision of Behavioral and Cognitive Neurology, Department of Neurology, Massachusetts General Hospital, Boston, Massachusetts
eHenry and Allison McCance Center for Brain Health, Massachusetts General Hospital, Boston, Massachusetts
*Corresponding author: Michael D. Kritzer, MD, PhD, Department of Psychiatry, Massachusetts General Hospital, 55 Fruit St, Boston, MA 02114 ([email protected]).
Frontotemporal neurocircuitry modulates cognitive and affective brain processes facilitating many aspects of mood, memory, and language, as well as social and executive functioning. Cortico-striatal neurocircuitry, connecting the frontal and temporal lobes to the thalamus, has been shown to coordinate many of these functions. Contributions from the anterior cingulate, orbitofrontal, medial and lateral prefrontal cortices, and insular cortex connect with limbic structures within the temporal lobes such as the amygdala, hippocampus, and parahippocampal gyrus to integrate multiple brain processes needed to plan and organize goal-directed behavior, as well as attach emotional valence to memory.
Infectious lesions can disrupt neurocircuitry causing loss of function.1 After the acute infection and treatment, long-standing sequelae may remain. The neuropsychiatric manifestations of these perturbations range from subtle to disabling, are often long-lasting, and profoundly affect the quality of life of patients and their families/caregivers. Infectious lesions may temporarily or permanently disrupt information processing in various brain regions. Compensatory neuroplasticity can be inadequate depending on the degree of tissue involved by the lesion and the age of the patient at onset of illness.
In this case series, we present 3 cases that underscore the need for awareness of long-lasting neuropsychiatric complications of brain infections. Two of the 3 cases involve sequelae from neuroinfectious diseases not often seen in the US. These patients presented decades after initial infection and respective immigration to the US. As health care providers, recognizing and treating such sequelae is our responsibility. In the US, societal biases combined with language and cultural barriers reduce the likelihood that people will present for care. Immigrants often enter the US with lower socioeconomic status, speak a different language, are isolated from their support infrastructure, can be stigmatized, and may express sentiment of objective or subjective discrimination as well as mistrust in the US medical system.2 Social determinants of health impact access to timely evaluation and treatment around the world.3 Providers trained in the US would benefit from cultural sensitivity training to lower barriers to treatment. These are important factors to consider when treating patients from other countries of origin.
Case 1
The first patient, a 47-year-old Ecuadoran woman with a 25-year history of neurocysticercosis (NCC) and epilepsy, presented to the Massachusetts General Hospital Behavioral Neurology Outpatient Clinic with mild depression, worsening anxiety, and impaired memory alongside word-finding and attentional difficulties 3 months after surgery for a cavernous malformation hemorrhage. She had undergone treatment for epilepsy secondary to NCC 25 years ago. She immigrated to the US at 27 years old and worked for a cleaning service company. At age 46, she presented to her primary care physician complaining of decreased short-term memory, “blanking out,” “losing [her] train of thought,” increased distractibility, and inattention combined with increased unexplained anxiety with heart palpitations. Her Montreal Cognitive Assessment (MoCA)4 score at that time was 20/30 with visuospatial (2/5) and delayed recall deficits (2/5) as well as serial 7s and fluency deficits. This result prompted brain magnetic resonance imaging (MRI) and subsequent neurosurgery for a cavernous malformation hemorrhage in her right middle temporal gyrus. Antiepileptic treatment had been discontinued 6 years prior to surgery given absence of generalized tonic-clonic seizures for 20 years (for timelines of case presentations, see Figure 1).
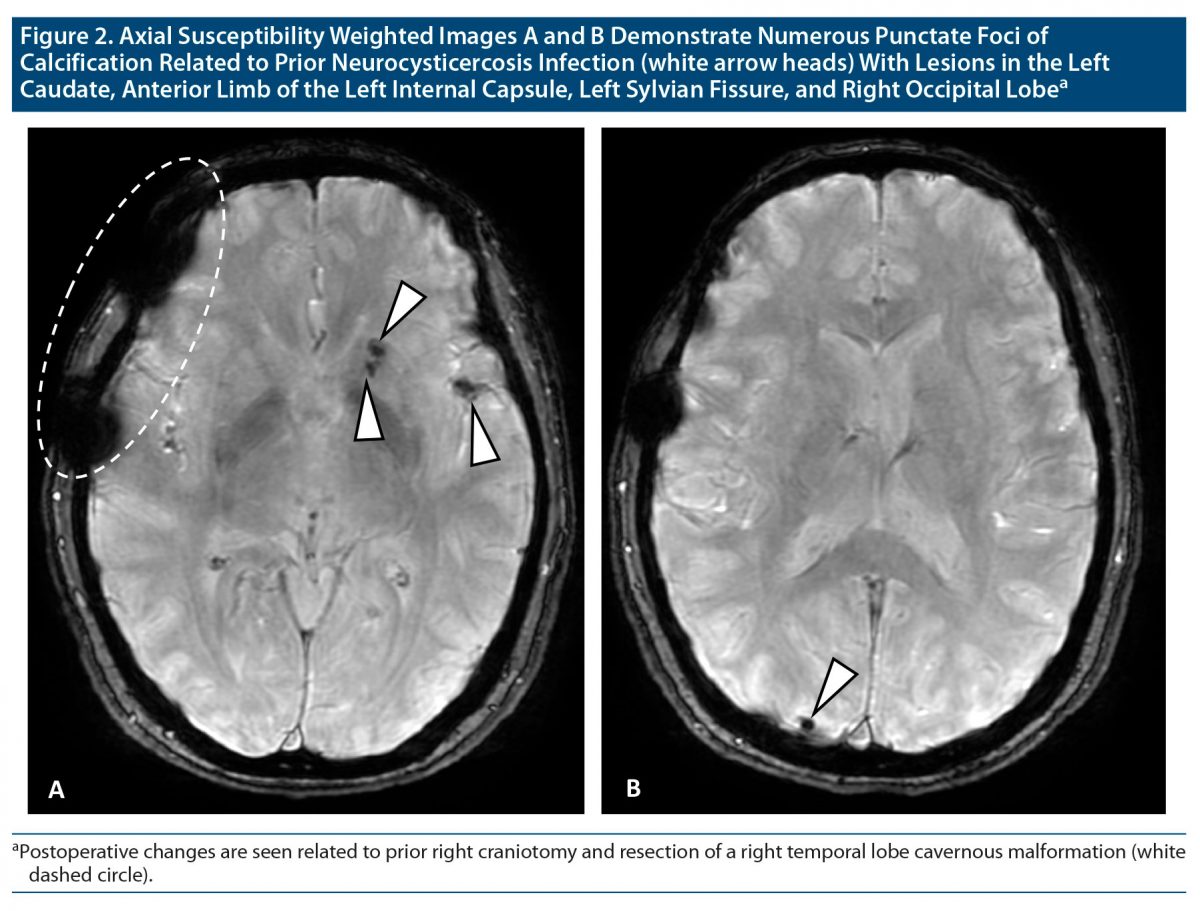
When we met, she was generally euthymic, though increasingly frustrated at her inability to recall details of events, needing people to repeat things for her, and forgetting whether or not she completed tasks a few minutes prior. Her brain MRI showed recent surgical changes related to the resection of her right cavernous malformation. It also revealed multiple calcified lesions consistent with her infection and treatment for NCC. She had lesions in her right occipital lobe, anterior paramedian right frontal parafalcine area, and the anterior limb of the left internal capsule that connects the thalamus to the frontal lobe (Figure 2). Her electroencephalogram (EEG) confirmed frequent left frontotemporal lobe epileptiform discharges. Given those findings, we restarted carbamazepine, and over the subsequent months, her symptoms improved. Her MoCA score had a net slight increase from 23/30 to 24/30 over the 6-month treatment period, notably with improvements in fluency (from 5 to 11 “F words”) and delayed recall (from 2/5 to 4/5). She lost 1 point in digit span during the second examination. The other aspects of the MoCA were unchanged, including deficits in cube drawing and repetition, though some language aspects may have been confounded by English being her second language.
While rare in the US, cysticercosis is endemic in many regions of the world, affecting over 50 million people worldwide, with predominance in Central and South America.5 The Infectious Diseases Society of America6 recommends treatment with albendazole for at least 14 days with or without the addition of praziquantel and monitoring for hepatotoxicity and leukopenia. NCC is a leading cause of acquired epilepsy worldwide, manifesting as seizures in up to 90% of cases and accounting for 2% of emergency department presentations in the US.7 Years after treatment of the acute infection, calcifications are typically present on neuroimaging studies and are not thought to have viable parasites,8 though epileptic foci may remain.9 Other symptoms include headaches, nausea, vomiting, psychosis, altered mental status, and cranial nerve palsies or other focal findings.10,11 Patients may experience vague subjective symptoms that are difficult to characterize, such as fatigue, decreased working or episodic memory, and attention, thus leading to prolonged morbidity. Initial workup would include brain MRI and EEG. Pharmacotherapy is used to target symptoms, and anticonvulsants are prescribed for patients with seizures. Generally, the seizures are fairly well controlled with medication and appropriate medical follow-up.12 Our patient, as many do,13–15 remained on antiepileptic therapy for decades after initial NCC treatment.
Case 2
The second patient, a 69-year-old Moroccan woman with vitamin B12 deficiency, hypertension, and diabetes presented with persistent cognitive complaints a year after completing chemotherapy for colon cancer and a course of antibiotic treatment for presumed neurosyphilis after having a positive syphilis antibody screen and RPR (rapid plasma reagin). She had immigrated as a young adult, having no formal education and 1 sexual partner who she had been married to for decades. She recalled being treated for a sexually transmitted disease 3 decades ago and understood it to be a result of her husband’s infidelity.
She presented to the Massachusetts General Hospital Behavioral Neurology Outpatient Clinic with depression and a history of “paranoia,” which was described as a relentless anxiety and catastrophizing with delusional aspects that would often bring her to panic—she would become concerned that her children living abroad were injured or dying with little reassurance until she spoke with them. As a consequence of short-term memory loss, this was an almost daily occurrence. She sometimes heard a voice calling her name. She also displayed mood lability with spontaneous crying as well as poor balance. She suffered from deficits in memory for faces, names, and details when conversing. She also had visuospatial and executive deficits—she would get lost in familiar places and could no longer use bus routes or follow a recipe. She was dependent on family for instrumental activities of daily living (IADLs) and increasingly for her ADLs. Her neurologic examination revealed a cautious gait and mild deficits in tandem gait, possibly caused by sensory loss (light touch and vibration) up to her knees. While she completed intravenous penicillin G for 14 days 1 year prior for presumed neurosyphilis (refusing a lumbar puncture), she did not receive a dose of intramuscular benzylpenicillin following completion of penicillin G, which was recommended by her infectious disease expert.
Her neuropsychological testing reflected a major neurocognitive disorder based on multidomain cognitive impairment in the context of significant compromise to her functional status. She was unable to count from 1 to 10. She correctly named a chair and a clock; she was unable to name a pencil but indicated that it is for writing. Her performances were extremely low across all measures of the Repeatable Battery Assessment of Neuropsychological Status,16 which included immediate memory (list learning, story memory, and visuospatial/constructional memory), semantic and fluent language, delayed recall, and attention with digit span.
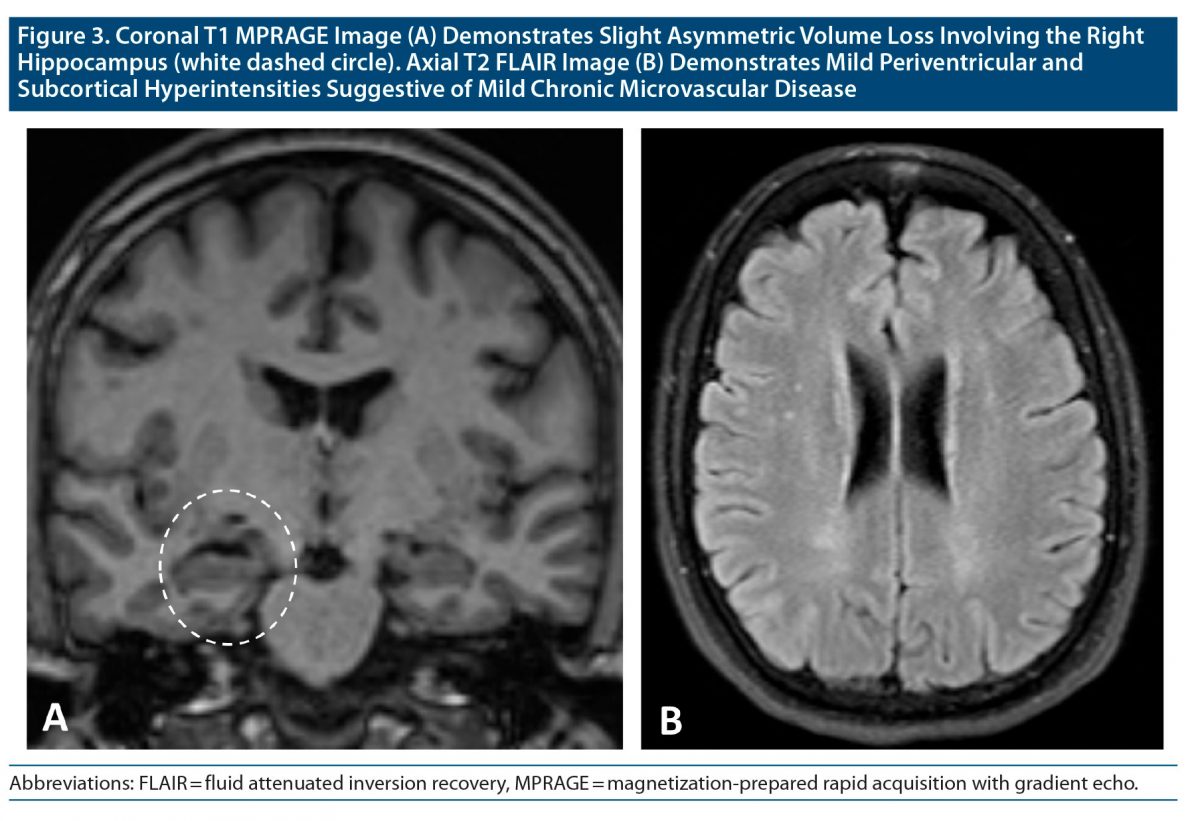
Her brain MRI showed white matter disease with mild anterior temporal lobe and hippocampal atrophy (right > left), though not much worse than expected for age (Figure 3). Her clinical presentation was far worse than her MRI revealed. The etiology of her cognitive, affective, and gait impairments was likely multifactorial and a consequence of a combination of neurosyphilis, vitamin B12 deficiency, chemotherapy, and white matter disease from hypertension and poorly controlled diabetes. Given her paranoia, amnesia, and visuospatial deficits, Alzheimer’s disease was also considered. Her mild hippocampal atrophy would be indicative of early disease, though her functional deficits appeared advanced. It was also possible that her confusion and memory complaints were secondary to partial seizures. We recommended intramuscular vitamin B12 injections, an EEG, which she failed to obtain, as well as a positron emission tomography (PET) scan and lumbar puncture, which she refused, and we are awaiting her follow-up.
Syphilis infection incidence is rising in the US.17 Neurosyphilis occurs in about 25%–40% of persons not treated for primary syphilis when the bacteria Treponema pallidum reaches the brain, meninges, and/or spinal cord.18,19 Appropriate diagnosis of neurosyphilis can be challenging, as this “great imitator” has various neurologic presentations.20–22 The clinical picture of subacute meningovascular syphilis, the most common form of neurosyphilis, may be associated with focal neurologic signs of cerebral arteritis.23 Late neurosyphilis has more widespread and less specific neuropsychiatric manifestations such as depression, confusion, dementia, apathy, emotional lability, and paranoid delusions.24–26 There are reports of temporal lobe atrophy27 and asymmetric mesiotemporal T2 hyperintense lesions on MRI images of the brain in neurosyphilis, and some lesions have even decreased with treatment.26,28–30 The MRI in our second case displayed mild asymmetric mesiotemporal atrophy (right > left) and white matter disease attributed to diabetes that may have been exacerbated by neurosyphilis infection. Additionally, neurosyphilis can manifest as seizures and was the presenting symptom in 12% of cases.31 These seizures may be focal or generalized.32 Nonconvulsive, unilateral, partial seizures, particularly in the frontal lobe, may not manifest in an obvious manner. Initial workup would include serologic testing for syphilis, then EEG if nonspecific frontal lobe symptoms persist, and brain MRI to assess any degree of atrophy. Suspicions regarding a diagnosis of Alzheimer’s disease can now be confirmed with a lumbar puncture,33 which can also be helpful in diagnosis of neurosyphilis.34
Case 3
The third patient presented to the Massachusetts General Hospital Neuropsychiatry Outpatient Clinic 40 years after an intensive care unit stay for septicemia and meningitis secondary to a foot infection. His first visit to the clinic 8 years ago revealed a 70-year-old White man with a decades-long history of depression with paranoia, irritability, rumination, anxiety with profound inability to make decisions (eg, whether or not to water his lawn caused a great deal of angst), and word-finding and memory difficulties. His wife accompanied him and did much of the talking. His neuropsychiatric sequelae, namely depression with paranoia and memory deficits, had worsened over the years, and his recurrent paranoid/ruminative symptoms were often linked to living in Florida annually during the winter.
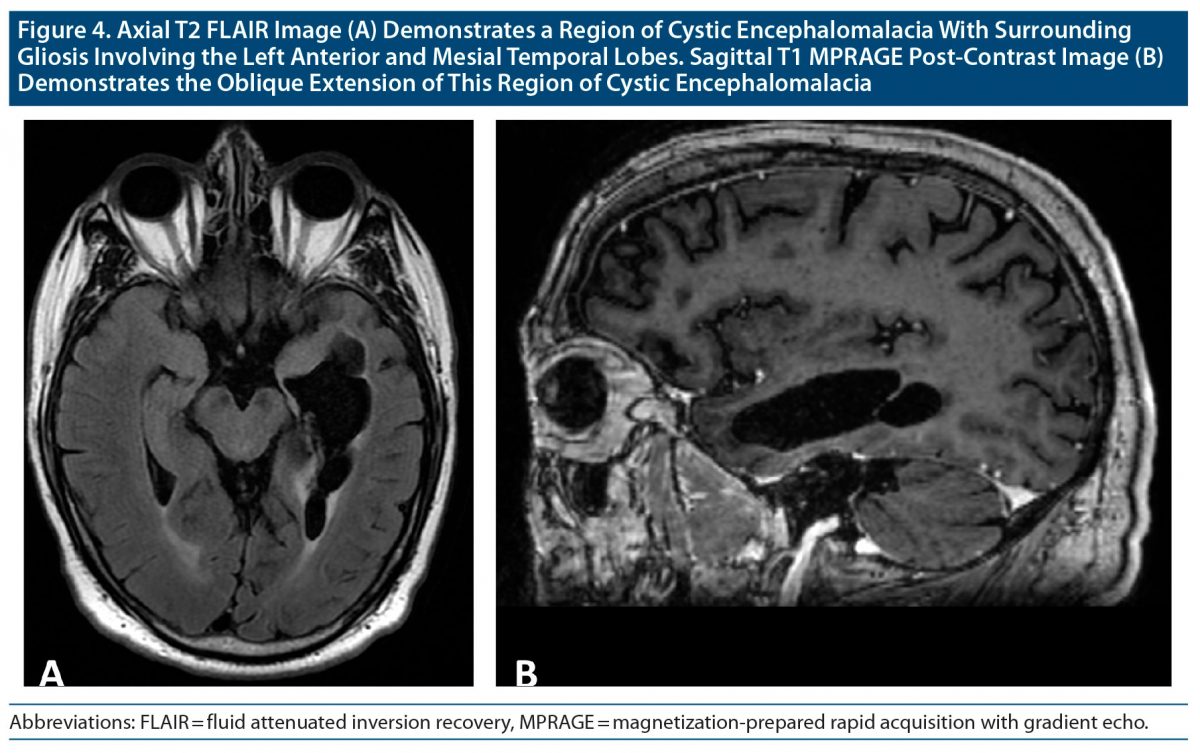
His cognitive examinations displayed persistent temporal lobe deficits, mainly difficulties with word retrieval and memory. His MoCA score was 24/30 in 2013 and had been stable at 25/30 since then with deficits in delayed recall including difficulties with retrieval and some decay with false positives. Then, he suffered from a severe episode of depression with neurovegetative symptoms and heightened paranoia in 2018 for which multiple antidepressant medication trials and augmentation using mirtazapine and the antipsychotics quetiapine and aripiprazole had no clinical benefit. His brain MRI in 2018 showed left temporal lobe encephalomalacia from a relatively large brain abscess (Figure 4). After 2 recent episodes of speech arrest, he was evaluated for seizures. His EEG revealed intermittent left frontal-temporal irregular-to-semirhythmic delta slowing and frequent left temporal > frontal epileptiform discharges. Lamotrigine was added to his medication regimen. Currently, his mood and psychotic symptoms are well controlled with duloxetine and low-dose olanzapine at night.
A brain abscess occurs due to a focal infection, typically hematogenously spread from a primary infection (eg, sinusitis, oral/dental, or pulmonary infections) or physical trauma or secondarily spread from previous brain surgery.35 Although up to 40% of brain abscesses may be cryptogenic with no identifiable cause, there are predisposing factors such as diabetes and illnesses that suppress the immune system (HIV, lupus, and chemotherapy). Advances in brain imaging, surgical technique, postsurgical care, duration of antibiotic administration, and surveillance have reduced the incidence. The incidence of brain abscesses is estimated to be between 0.3 and 1.3 per 100,000 people per year.36 Brain abscesses are life-threatening and may still lead to permanent neuropsychiatric symptoms even after appropriate treatment. In recent decades, mortality and morbidity have improved to 13.6% and 6.3%, respectively.37 Depending on the location of the lesion, patients may experience depression, apathy, memory impairment, and visuospatial, word-finding, attentional, and/or executive deficits, and these may persist and evolve for decades, requiring ongoing treatment. Seizures have been shown in patients as a presenting symptom for, and when recovering from, brain abscess surgery. There is varied incidence with a range of 6.4%–43%, though up to 70% of people with a history of brain abscess have a seizure within a 30-year follow-up. Most practitioners recommend anticonvulsant therapy for 5 years following brain abscess, and then a cessation trial is appropriate.38 Initial workup should include brain MRI and EEG if symptoms persist.
Frontotemporal Neurocircuitry in Cognitive and Affective Processing
Historically, we have learned a great deal of functional neuroanatomy from well-characterized patients suffering from lesions involving the frontal lobe, thereby altering cognitive and affective processing. The patient known as Phineas Gage lost the function of his left orbitofrontal region after an accident while tamping railroad stakes resulting in changes to his degree of sociability, irritability, and impulsivity.39,40 The patient known as Henry Molaison (previously known as patient H.M.) had iatrogenic bilateral resection of the anterior two-thirds of his hippocampi, amygdala, and parahippocampal, entorhinal, and piriform cortices to treat his intractable epilepsy. As a result, he became amnestic to novel experiences (anterograde) as well as suffered from temporally graded retrograde amnesia.41,42 Additionally, brain areas involving language deficits reflect well-known monikers belonging to Broca and Wernicke for lesions to the frontal and temporal lobe, respectively, although these regions are not as circumscribed as previously thought.43–46 While the future of functional neuroanatomy may be understood as distributed neural networks through results from functional MRI (fMRI)47,48 and diffusion tensor imaging,49 longitudinal assessments of patients with brain lesions can provide clinically relevant, neuroanatomically informed, and patient-centered formulations for treatment and rehabilitative approaches.
The frontal lobes provide the ability to learn, plan, and execute complex cognitive, affective, and behavioral tasks. Frontal lobes orchestrate executive functions such as attention, working memory, decision-making, and sociability, as well as enable inhibitory control over impulses.39,50 The temporal lobes are associated with language, though that is typically lateralized to the left hemisphere. The temporal lobes also house many limbic and paralimbic structures bilaterally such as the amygdala, hippocampus, and parahippocampal gyrus, which associates emotion with experience.51,52 Direct connections between the frontal and temporal lobes likely facilitate working and episodic memory as well as emotional processing, social cognition, and self-awareness. The frontal and temporal lobes are connected indirectly through thalamic relay connections and directly via the uncinate fascicle (UF), a white matter bundle that connects the anterior temporal lobe with the frontal cortex bilaterally.53 The UF belongs to the limbic system, connecting the amygdala, hippocampal formation, anterior temporal convexity, temporal and frontal poles, frontal basal area, and inferior frontal gyrus (mainly the orbitofrontal cortex). The UF has been implicated in emotional processing, memory, behavioral responses, social cognition, and language.52–57 Additionally, the internal capsule is a white matter bundle that connects the cerebral cortex with subcortical structures bilaterally58 and connects the frontal lobe to the thalamus.59 The thalamus, known as the gateway to the cortex, integrates and relays cognitive and sensory information including pain, motor signals, consciousness, and arousal as well as mediates self-awareness.60,61
Two recent meta-analyses62,63 of task-related fMRI experiments detected robust patterns of brain activity across various psychiatric disorders. The first study by Janiri et al62 investigated stress-related disorders and found overlapping clusters of hypo- and hyperactivation of brain regions in mood disorders, posttraumatic stress disorder, and anxiety disorders. They found hypoactivation of a right-dominant brain system, specifically in the inferior prefrontal cortex/insula, the inferior parietal lobule, and the putamen—regions that support context shifting and inhibition of some mental operations and behavioral responses. The right inferior prefrontal cortex and right putamen are involved in the inhibition of contextually inappropriate cognitive, affective, and motor responses. The authors62 inferred that there was transdiagnostic disruption in salience processing (including interoceptive processing) and inhibitory control. They also identified transdiagnostic clusters of hyperactivation in the left amygdala/parahippocampal gyrus, the left thalamus, and the perigenual/dorsal anterior cingulate cortex relating to affective and social processing. The second meta-analysis63 of task-related data had a broader selection of psychiatric illness by including individuals with schizophrenia and substance use disorders in addition to mood and anxiety disorders. Although some of the source data likely overlaps between these 2 studies, McTeague et al63 also found that nonpsychotic disorders displayed hyperactivation of the left amygdala and dorsolateral thalamus and hypoactivation in the ventromedial and right ventrolateral prefrontal cortex; however, they found the opposite with respect to the dorsal anterior cingulate cortex. This line of evidence further implicates frontotemporal regions in the regulation of cognitive and affective processes.
Over recent years, a few meta-analyses have been conducted on studies evaluating resting-state fMRI in psychiatric disorders, including major depressive disorder (MDD), anxiety disorder, obsessive-compulsive disorder, and posttraumatic stress disorder.64–67 As opposed to task-based fMRI, resting-state fMRI evaluates brain activity when a subject is not engaged in a specific task. This approach seeks to determine what the brain is doing at rest. Kaiser and colleagues64 found that patients with MDD displayed hypoconnectivity within the frontoparietal network, a set of brain regions involved in attention and emotion regulation, as well as the salience network (SN), comprised mainly of the anterior cingulate and anterior insula, that facilitates top-down regulation of those functions. MDD was also associated with hyperconnectivity within the default mode network (DMN), a network made up of the medial prefrontal cortex, the posterior cingulate/precuneus, and the angular gyrus believed to support internally oriented and self-referential thought, wherein increased activity correlates with cognitive ruminations.64 Additionally, a meta-analysis65 of anxiety disorders revealed hypoconnectivity of the executive control network—mainly the dorsolateral prefrontal cortex (DLPFC) and posterior parietal cortex—with the DMN. The connectivity within the SN itself and its connectivity with the sensorimotor network were also decreased.65 These results illustrate consistent dysregulations of affective and cognitive control-related networks involving the PFC and connected structures in depressive and anxiety disorders.
Our first patient presented with a history of NCC with lesions in her right occipital lobe, anterior paramedian right frontal parafalcine area, and the anterior limb of the left internal capsule and endorsed worsening mood and anxiety as well as frustration about her cognitive symptoms. While this could be secondary to the cognitive difficulties (attention and working memory), it could also be primary, as lesions to the left DLPFC have been shown to increase affective symptoms and antidepressant treatment increases DLPFC activity.68–70 Her inattention and word-finding and working memory deficits were likely explained by the epileptiform activity in her left frontal lobe.71 Additionally, neurologic processing of internal body state and external environmental information traverses the internal capsule, which connects the frontal lobes and the thalamus. She had a lesion in the left anterior internal capsule as well as left frontotemporal epileptiform discharges likely disrupting frontal-thalamic neurocircuitry and contributing to her inability to attend to appropriate stimuli, task shift, and recall. This improved with the reinitiation and titration of her antiepileptic medication. Disruptions in this neurocircuitry likely contributed to her overall symptomatology, though there has probably been some degree of compensatory neuroplasticity over the past 25 years. Her MoCA score was largely consistent with a frontotemporal impairment in working memory, attention, and language and difficulties with word recall.
The MRI of our second patient displayed mild mesiotemporal atrophy (Figure 3). The reduction in the cells connecting mesiotemporal structures such as the hippocampus, parahippocampal gyrus, and amygdala to the inferior frontal lobe structures such as the orbitofrontal cortex likely contributed to her amnestic dementing process and inability to appropriately control her affective symptoms. Lastly, our third patient displayed episodic and gradually worsening difficulties with emotion regulation and cognition—his depression with psychosis, word-finding difficulties, and memory loss. This can at least be partly explained by the impaired connection between his left anterior temporal pole with brain structures involved in the neurocircuitry of language, working memory, and inhibitory control of affect—mainly the anterior cingulate and orbitofrontal cortices along with the amygdala and hippocampus. He also had left temporal > frontal epileptiform discharges that had not been adequately controlled over the years. His MRI displayed encephalomalacia of the left anterior and mesial temporal lobes (Figure 4). He was missing white matter in this region and therefore was missing the connections between much of his temporal lobe to subcortical and frontal brain regions. This lesion was responsible for his word-finding deficits and likely his challenges in working memory and attention. He was missing his left UF and consequently the bilateral subcortical connections to the frontal lobes, including the orbitofrontal cortices, known to help regulate impulses and emotion as well as assign value to thoughts and experiences.
Though differing substantially in their etiology, a theme emerged from these 3 cases as their brain lesions precipitated deficits in cognition manifesting in symptoms such as confusion, inattention, and trouble with working memory and word-finding as well as affective symptoms of mood instability, depression, and anxiety. These symptoms are often difficult to assess clinically, and when combined with cultural consequences of immigration, it is likely that delays in evaluation and treatment will occur and adversely affect an individual’s quality of life. Although prevention and access to treatment have decreased the incidence of neuroinfectious diseases in the US, primary care providers would benefit from being familiar with their occurrence, neuropsychiatric presentation, evaluation, and treatment.
Published online: November 4, 2021.
Potential conflicts of interest: None.
Funding/support: Support was received from the Massachusetts General Hospital T32 Translational Neuroscience Training for Clinicians (T32MH112485) training grant (Dr Kritzer).
Role of the sponsor: The sponsor had no role in the design and conduct of the study; collection, management, analysis, and interpretation of data; or preparation, review or approval of the manuscript.
Patient consent: Authorization for publication was obtained by each patient or their next of kin prior to the submission of this case series. Information has been de-identified to protect anonymity.
Author Affiliations

- Division of Neuropsychiatry, Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts
- Corresponding author: Michael D. Kritzer, MD, PhD, Department of Psychiatry, Massachusetts General Hospital, 55 Fruit St, Boston, MA 02114 ([email protected]).
- Department of Radiology, Massachusetts General Hospital, Boston, Massachuetts
- Department of Neurology, Massachusetts General Hospital, Boston, Massachuetts
- Division of Neuropsychiatry, Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts
- Division of Behavioral and Cognitive Neurology, Department of Neurology, Massachusetts General Hospital, Boston, Massachuetts
- Henry and Allison McCance Center for Brain Health, Massachusetts General Hospital, Boston, Massachuetts
- Division of Neuropsychiatry, Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts
- Department of Neurology, Massachusetts General Hospital, Boston, Massachuetts
- Division of Behavioral and Cognitive Neurology, Department of Neurology, Massachusetts General Hospital, Boston, Massachuetts
- Henry and Allison McCance Center for Brain Health, Massachusetts General Hospital, Boston, Massachuetts
References (71)
- Munjal S, Ferrando SJ, Freyberg Z. Neuropsychiatric aspects of infectious diseases: an update. Crit Care Clin. 2017;33(3):681–712. PubMed CrossRef
- Menjívar C, Cervantes AG. Immigration. In: Treviño AJ, ed. The Cambridge Handbook of Social Problems. 2018.
- Singh GK, Daus GP, Allender M, et al. Social determinants of health in the United States: addressing major health inequality trends for the nation, 1935–2016. Int J MCH AIDS. 2017;6(2):139–164. PubMed CrossRef
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. PubMed CrossRef
- White AC Jr. Neurocysticercosis: a major cause of neurological disease worldwide. Clin Infect Dis. 1997;24(2):101–113, quiz 114–115. PubMed CrossRef
- White AC Jr, Coyle CM, Rajshekhar V, et al. Diagnosis and treatment of neurocysticercosis: 2017 clinical practice guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Am J Trop Med Hyg. 2018;98(4):945–966. PubMed CrossRef
- Ong S, Talan DA, Moran GJ, et al; EMERGEncy ID NET Study Group. Neurocysticercosis in radiographically imaged seizure patients in US emergency departments. Emerg Infect Dis. 2002;8(6):608–613. PubMed CrossRef
- Sarria Estrada S, Frascheri Verzelli L, Siurana Montilva S, et al. Imaging findings in neurocysticercosis [in Spanish]. Radiologia (Madr). 2013;55(2):130–141. PubMed CrossRef
- Medina MT, Dubón-Murcia SA, Aguilar-Estrada RL, et al. Neurocysticercosis and epilepsy. Epilepsies. 2010;22(2):126–133. CrossRef
- García HH, Gonzalez AE, Evans CAW, et al; Cysticercosis Working Group in Peru. Taenia solium cysticercosis. Lancet. 2003;362(9383):547–556. PubMed CrossRef
- Siddiqua T, Habeeb A. Neurocysticercosis. Saudi J Kidney Dis Transpl. 2020;31(1):254–258. PubMed CrossRef
- Del Brutto OHD, Santibañez R, Noboa CA, et al. Epilepsy due to neurocysticercosis: analysis of 203 patients. Neurology. 1992;42(2):389–392. PubMed CrossRef
- Nash TE, Mahanty S, Loeb JA, et al. Neurocysticercosis: a natural human model of epileptogenesis. Epilepsia. 2015;56(2):177–183. PubMed CrossRef
- Del Brutto OH, Engel J Jr, Eliashiv DS, et al. Update on cysticercosis epileptogenesis: the role of the hippocampus. Curr Neurol Neurosci Rep. 2016;16(1):1. PubMed CrossRef
- Garcia HH. Neurocysticercosis. Neurol Clin. 2018;36(4):851–864. PubMed CrossRef
- Randolph C, Tierney MC, Mohr E, et al. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): preliminary clinical validity. J Clin Exp Neuropsychol. 1998;20(3):310–319. PubMed CrossRef
- Schmidt R, Carson PJ, Jansen RJ. Resurgence of syphilis in the United States: an assessment of contributing factors. Infect Dis (Auckl). 2019;12:1178633719883282. PubMed CrossRef
- Holland BE. Neurosyphillis. J Nerv Ment Dis. 1926;63(2):181. CrossRef
- Özselek S, Erdem M, Uzun Ö, et al. A neurosyphilis case presenting with dementia. Dusunen Adam. 2011;24:145–148. CrossRef
- Domantay-Apostol GP, Handog EB, Gabriel MTG. Syphilis: the international challenge of the great imitator. Dermatol Clin. 2008;26(2):191–202, v. PubMed CrossRef
- Yanhua W, Haishan S, Le H, et al. Clinical and neuropsychological characteristics of general paresis misdiagnosed as primary psychiatric disease. BMC Psychiatry. 2016;16(1):230. PubMed CrossRef
- Militz H, Hungerer C. Images in clinical medicine. treponema pallidum—the great imitator.. N Engl J Med. 2015;373(21):2069. PubMed CrossRef
- Chahine LM, Khoriaty RN, Tomford WJ, et al. The changing face of neurosyphilis. Int J Stroke. 2011;6(2):136–143. PubMed CrossRef
- Jay CA. Treatment of neurosyphilis. Curr Treat Options Neurol. 2006;8(3):185–192. PubMed CrossRef
- Jantzen SU, Ferrea S, Langebner T, et al. Late-stage neurosyphilis presenting with severe neuropsychiatric deficits: diagnosis, therapy, and course of three patients. J Neurol. 2012;259(4):720–728. PubMed CrossRef
- Mehrabian S, Raycheva M, Traykova M, et al. Neurosyphilis with dementia and bilateral hippocampal atrophy on brain magnetic resonance imaging. BMC Neurol. 2012;12(1):96. PubMed CrossRef
- Nagappa M, Sinha S, Taly AB, et al. Neurosyphilis: MRI features and their phenotypic correlation in a cohort of 35 patients from a tertiary care university hospital. Neuroradiology. 2013;55(4):379–388. PubMed CrossRef
- Jeong YM, Hwang HY, Kim HS. MRI of neurosyphilis presenting as mesiotemporal abnormalities: a case report. Korean J Radiol. 2009;10(3):310–312. PubMed CrossRef
- Hama K, Ishiguchi H, Tuji T, et al. Neurosyphilis with mesiotemporal magnetic resonance imaging abnormalities. Intern Med. 2008;47(20):1813–1817. PubMed CrossRef
- Bash S, Hathout GM, Cohen S. Mesiotemporal T2-weighted hyperintensity: neurosyphilis mimicking herpes encephalitis. AJNR Am J Neuroradiol. 2001;22(2):314–316. PubMed
- Punia V, Marks D. Clinical and eeg characteristics of seizure disorders in neurosyphilis. Neurology. 2013;80(7 suppl):P07.174.
- Marano E, Briganti F, Tortora F, et al. Neurosyphilis with complex partial status epilepticus and mesiotemporal MRI abnormalities mimicking herpes simplex encephalitis. J Neurol Neurosurg Psychiatry. 2004;75(6):833. PubMed CrossRef
- Blennow K, Dubois B, Fagan AM, et al. Clinical utility of cerebrospinal fluid biomarkers in the diagnosis of early Alzheimer’s disease. Alzheimers Dement. 2015;11(1):58–69. PubMed CrossRef
- Marra CM, Maxwell CL, Smith SL, et al. Cerebrospinal fluid abnormalities in patients with syphilis: association with clinical and laboratory features. J Infect Dis. 2004;189(3):369–376. PubMed CrossRef
- Brouwer MC, Tunkel AR, McKhann GM 2nd, et al. Brain abscess. N Engl J Med. 2014;371(5):447–456. PubMed CrossRef
- Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology. 2014;82(9):806–813. PubMed CrossRef
- Prasad KN, Mishra AM, Gupta D, et al. Analysis of microbial etiology and mortality in patients with brain abscess. J Infect. 2006;53(4):221–227. PubMed CrossRef
- Patel K, Clifford DB. Bacterial brain abscess. Neurohospitalist. 2014;4(4):196–204. PubMed CrossRef
- Zald DH, Rauch SL. The Orbitofrontal Cortex. Oxford University Press; 2010.
- Tobia KP. Phineas Gage. In: The Curated Reference Collection in Neuroscience and Biobehavioral Psychology. Elsevier, Inc; 2016.
- Squire LR. The legacy of patient H.M. for neuroscience. Neuron. 2009;61(1):6–9. PubMed CrossRef
- Eichenbaum H. What H.M. taught us. J Cogn Neurosci. 2013;25(1):14–21. PubMed CrossRef
- Poeppel D, Hickok G. Towards a new functional anatomy of language. Cognition. 2004;92(1–2):1–12. PubMed CrossRef
- Hagoort P. On Broca, brain, and binding: a new framework. Trends Cogn Sci. 2005;9(9):416–423. PubMed CrossRef
- Mohr JP, Pessin MS, Finkelstein S, et al. Broca aphasia: pathologic and clinical. Neurology. 1978;28(4):311–324. PubMed CrossRef
- Fridriksson J, den Ouden DB, Hillis AE, et al. Anatomy of aphasia revisited. Brain. 2018;141(3):848–862. PubMed CrossRef
- Mumford JA, Ramsey JD. Bayesian networks for fMRI: a primer. Neuroimage. 2014;86:573–582. PubMed CrossRef
- Pervaiz U, Vidaurre D, Woolrich MW, et al. Optimising network modelling methods for fMRI. Neuroimage. 2020;211:116604. PubMed CrossRef
- Lope-Piedrafita S. Diffusion tensor imaging (DTI). In: García Martín M, López Larrubia P, eds. Preclinical MRI: Methods in Molecular Biology. 2018.
- Bemjamin S. The Human Frontal Lobes: Functions and Disorders, 2nd ed. J Clin Psychiatry. 2007;68(11):1817–1818. CrossRef
- Greenberg WM. Review of brain circuitry and signaling in psychiatry: basic science and clinical implications. Am J Orthopsychiatry. 2002;72(4):600–601. CrossRef
- Lin JJ, Riley JD, Juranek J, et al. Vulnerability of the frontal-temporal connections in temporal lobe epilepsy. Epilepsy Res. 2008;82(2–3):162–170. PubMed CrossRef
- Bracht T, Linden D, Keedwell P. A review of white matter microstructure alterations of pathways of the reward circuit in depression. J Affect Disord. 2015;187:45–53. PubMed CrossRef
- Schmahmann JD, Pandya DN, Wang R, et al. Association fibre pathways of the brain: parallel observations from diffusion spectrum imaging and autoradiography. Brain. 2007;130(pt 3):630–653. PubMed CrossRef
- de Kwaasteniet B, Ruhe E, Caan M, et al. Relation between structural and functional connectivity in major depressive disorder. Biol Psychiatry. 2013;74(1):40–47. PubMed CrossRef
- Hanlon FM, Houck JM, Klimaj SD, et al. Frontotemporal anatomical connectivity and working-relational memory performance predict everyday functioning in schizophrenia. Psychophysiology. 2012;49(10):1340–1352. PubMed CrossRef
- Ribas EC, Yagmurlu K, Wen HT, et al. Microsurgical anatomy of the inferior limiting insular sulcus and the temporal stem. J Neurosurg. 2015;122(6):1263–1273. PubMed CrossRef
- Bae JN, MacFall JR, Krishnan KRR, et al. Dorsolateral prefrontal cortex and anterior cingulate cortex white matter alterations in late-life depression. Biol Psychiatry. 2006;60(12):1356–1363. PubMed CrossRef
- Sullivan EV, Zahr NM, Rohlfing T, et al. Fiber tracking functionally distinct components of the internal capsule. Neuropsychologia. 2010;48(14):4155–4163. PubMed CrossRef
- Chien JH, Cheng JJ, Lenz FA. The Thalamus. In: Conn PM, ed. Conn’s Translational Neuroscience. Academic Press; 2017. doi:
- Haber SN, Calzavara R. The cortico-basal ganglia integrative network: the role of the thalamus. Brain Res Bull. 2009;78(2–3):69–74. PubMed CrossRef
- Janiri D, Moser DA, Doucet GE, et al. Shared neural phenotypes for mood and anxiety disorders: a meta-analysis of 226 task-related functional imaging studies. JAMA Psychiatry. 2020;77(2):172–179. PubMed CrossRef
- McTeague LM, Rosenberg BM, Lopez JW, et al. Identification of common neural circuit disruptions in emotional processing across psychiatric disorders. Am J Psychiatry. 2020;177(5):411–421. PubMed CrossRef
- Kaiser RH, Andrews-Hanna JR, Wager TD, et al. Large-scale network dysfunction in major depressive disorder: a meta-analysis of resting-state functional connectivity. JAMA Psychiatry. 2015;72(6):603–611. PubMed CrossRef
- Xu J, Van Dam NT, Feng C, et al. Anxious brain networks: a coordinate-based activation likelihood estimation meta-analysis of resting-state functional connectivity studies in anxiety. Neurosci Biobehav Rev. 2019;96:21–30. PubMed CrossRef
- Gürsel DA, Avram M, Sorg C, et al. Frontoparietal areas link impairments of large-scale intrinsic brain networks with aberrant fronto-striatal interactions in OCD: a meta-analysis of resting-state functional connectivity. Neurosci Biobehav Rev. 2018;87:151–160. PubMed CrossRef
- Koch SBJ, van Zuiden M, Nawijn L, et al. Aberrant resting-state brain activity in posttraumatic stress disorder: a meta-analysis and systematic review. Depress Anxiety. 2016;33(7):592–605. PubMed CrossRef
- Shackman AJ, McMenamin BW, Maxwell JS, et al. Right dorsolateral prefrontal cortical activity and behavioral inhibition. Psychol Sci. 2009;20(12):1500–1506. PubMed CrossRef
- Cisler JM, James GA, Tripathi S, et al. Differential functional connectivity within an emotion regulation neural network among individuals resilient and susceptible to the depressogenic effects of early life stress. Psychol Med. 2013;43(3):507–518. PubMed CrossRef
- Beall EB, Malone DA, Dale RM, et al. Effects of electroconvulsive therapy on brain functional activation and connectivity in depression. J ECT. 2012;28(4):234–241. PubMed CrossRef
- Barbey AK, Koenigs M, Grafman J. Dorsolateral prefrontal contributions to human working memory. Cortex. 2013;49(5):1195–1205. PubMed CrossRef
Enjoy free PDF downloads as part of your membership!
![]() Save
Save
![]() Share
Share
![]() Cite
Cite

