
Prim Care Companion CNS Disord 2022;24(4):22cr03300
To cite: Moideen S, Innisai A, Uvais NA. Bilateral olfactory bulb in post–COVID-19 parosmia. Prim Care Companion CNS Disord. 2022;24(4):22cr03300.
To share: https://doi.org/10.4088/PCC.22cr03300
© 2022 Physicians Postgraduate Press, Inc.
aDepartment of Internal Medicine, Iqraa International Hospital and Research Centre, Calicut, Kerala, India
bDepartment of Radiology, Iqraa International Hospital and Research Centre, Calicut, Kerala, India
cDepartment of Psychiatry and Health Research, Iqraa International Hospital and Research Centre, Calicut, Kerala, India
*Corresponding author: N. A. Uvais, MBBS, DPM, Iqraa International Hospital and Research Centre, Malaparamba, Calicut, Kerala 673009, India ([email protected]).
Olfactory dysfunction has been reported in a significant number of patients with coronavirus disease 2019 (COVID-19) infection.1 The most commonly reported olfactory dysfunctions among patients with active COVID-19 infections were anosmia (a total loss of smell) and hyposmia (a decrease in the sense of smell).1 The olfactory symptoms usually resolve with recovery in the majority of patients, indicating that the potential mechanism could be the local inflammation of the olfactory area on the roof of the nose.1,2
However, parosmia has been reported in a smaller number of patients with COVID-19 infection, which rarely has been found to persist for longer periods even after complete recovery from COVID-19 infection.2 One potential reason for the persistence of parosmia among COVID-19 survivors could be the invasion of the olfactory nervous system by the COVID-19 virus.1 Here, we report a case of persistent parosmia in an elderly women with magnetic resonance imaging (MRI) findings of bilateral olfactory bulb atrophy, supporting a neuronal mechanism for persisting olfactory symptoms among COVID-19 survivors.
Case Report
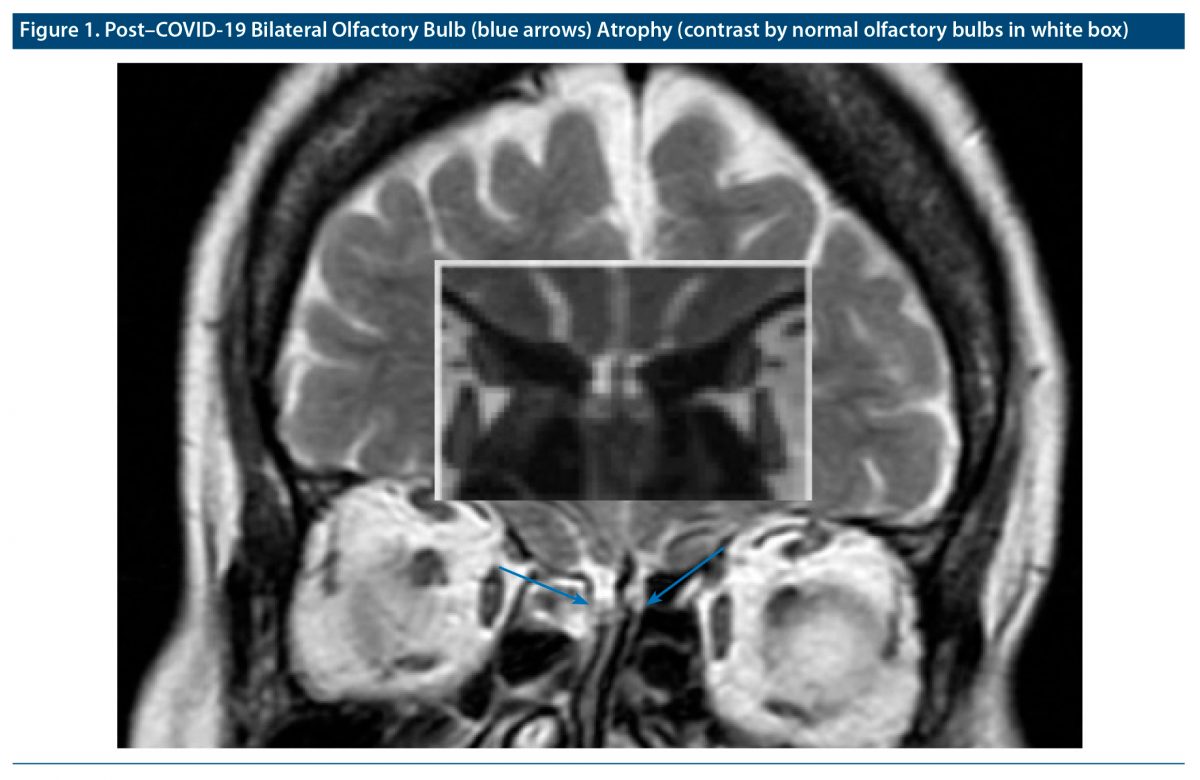
An asymptomatic 68-year-old woman was diagnosed with COVID-19 by reverse transcription polymerase chain reaction when she was tested due to close contact with symptomatic COVID-19–positive family members. She developed intolerable foul smell perception of cooked food items after 2 months of testing positive for COVID-19. Due to the foul smell, she preferred to stay outside her home and actively avoided going to restaurants and family functions. A 1.5T MRI, conducted after 2 months while parosmia was persisting, showed signs of bilateral olfactory bulb atrophy (Figure 1).
Discussion
Parosmia is characterized by olfactory distortion in the presence of an existing stimulus.1 There are various causes for parosmia reported in the literature, such as neurodegenerative disorders, traumatic brain injury, and nasal and sinus problems, as well as idiopathic disease.2 The COVID-19 virus has shown affinity for olfactory epithelium via angiotensin-converting enzyme 2 and transmembrane protease serine 2 receptors, leading to various olfactory symptoms including parosmia.2 A recent study3 reported that 64.1% of the respondents out of 148 individuals with olfactory dysfunction associated with laboratory-confirmed or clinically suspected COVID-19 infection reported parosmia at some point during or after COVID-19 infection, which significantly affected their quality of life. Another case series1 from Iraq reported COVID-19–associated parosmia was significantly higher among younger patients (aged < 30 years), females, housewives, and nonsmokers. None of the existing literature, to the best of our knowledge, reports olfactory bulb atrophy in post–COVID-19 parosmia. However, Chiu et al4 reported COVID-19 anosmia with definitive olfactory bulb atrophy compared with pre-COVID imaging in a 19-year-old female. Hence, this case highlights a neuroimaging finding in patients with post–COVID-19 parosmia, which has hitherto not been reported.
Received: April 2, 2022.
Published online: August 4, 2022.
Relevant financial relationships: None.
Funding/support: None.
Patient consent: Consent was received from the patient to publish the case report, and information has been de-identified to protect anonymity.
Author Affiliations

- Department of Internal Medicine, Iqraa International Hospital and Research Centre, Calicut, Kerala, India
- Department of Radiology, Iqraa International Hospital and Research Centre, Calicut, Kerala, India
- Department of Psychiatry and Health Research, Iqraa International Hospital and Research Centre, Calicut, Kerala, India
- Corresponding author: N. A. Uvais, MBBS, DPM, Iqraa International Hospital and Research Centre, Malaparamba, Calicut, Kerala 673009, India ([email protected]).
References (4)
- Rashid RA, Alaqeedy AA, Al-Ani RM. Parosmia due to COVID-19 disease: a 268 case series [published online ahead of print May 23, 2021]. Indian J Otolaryngol Head Neck Surg. 2021:1–8. PubMed CrossRef
- Duyan M, Ozturan IU, Altas M. Delayed parosmia following SARS-CoV-2 infection: a rare late complication of COVID-19 SN Compr Clin Med. 2021;3(5):1200–1202. PubMed CrossRef
- Lerner DK, Garvey KL, Arrighi-Allisan AE, et al. Clinical features of parosmia associated with COVID-19 infection. Laryngoscope. 2022;132(3):633–639. PubMed CrossRef
- Chiu A, Fischbein N, Wintermark M, et al. COVID-19–induced anosmia associated with olfactory bulb atrophy. Neuroradiology. 2021;63(1):147–148. PubMed CrossRef
Enjoy free PDF downloads as part of your membership!
![]() Save
Save
![]() Share
Share
![]() Cite
Cite



